This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria. The early HATW model correctly identifies the HATWs in the inferior leads.
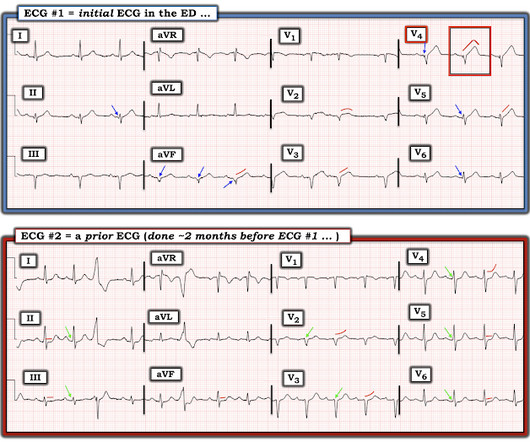
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
I simply texted back: "Definite posterior OMI." The person I was texting knows implicitly based on our experience together that I mean "Definite posterior OMI, assuming the patient's clinical presentation is consistent with ACS." The patient was a middle-aged female who had acute chest pain of approximately 6 hours duration.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
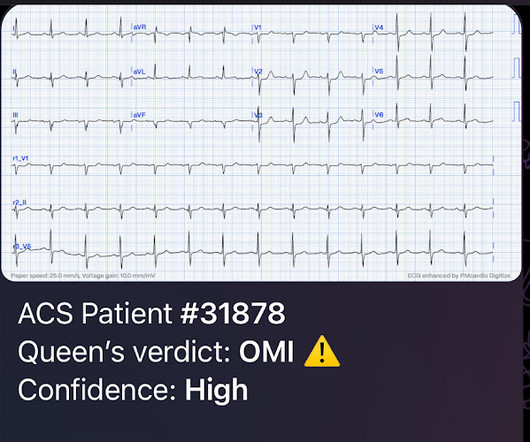
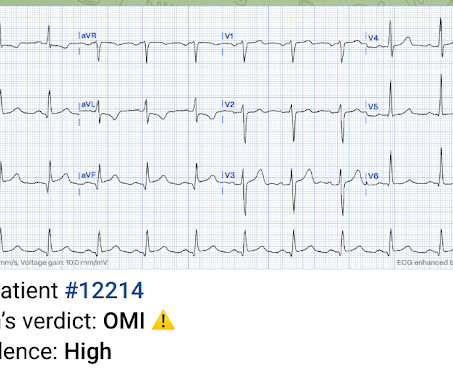
I sent this ECG to the Queen of Hearts (PMcardio OMI), and here is the verdict: You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form Then I learned that a Code STEMI was activated for concern of anterior "STEMI" in V1-V2. High sensitivity troponin I was 23 ng/L.
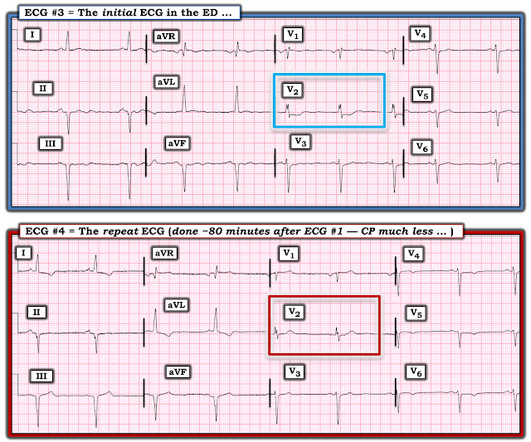
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. What lowered my confidence in calling ECG #1 a definite OMI — was the finding of somewhat similar-appearing , upright T waves with slight-but-real J-point ST elevation in so many leads ( ie, leads I,II,aVF; V2-thru-V6 ). What did I say?
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The article by Aslanger, Smith et al that is featured above in today’s post has just been published.
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." The patient was discharged home the next day. No further follow up is available.
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore, this does not meet the definition of myocardial infarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. You can see the deficiency of the definition of MI.
Objective: ST-elevation myocardial infarction (STEMI) is a leading cause of mortality in Australia. Paramedics treating adults with STEMI in the out-of-hospital environment can use fentanyl or morphine to manage the patient’s pain, although there is little research comparing the efficacy and safety of these drugs.
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
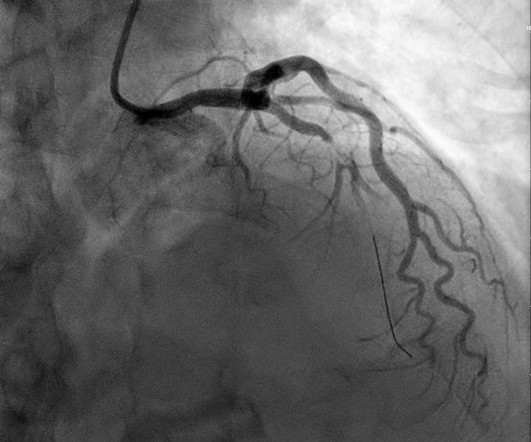
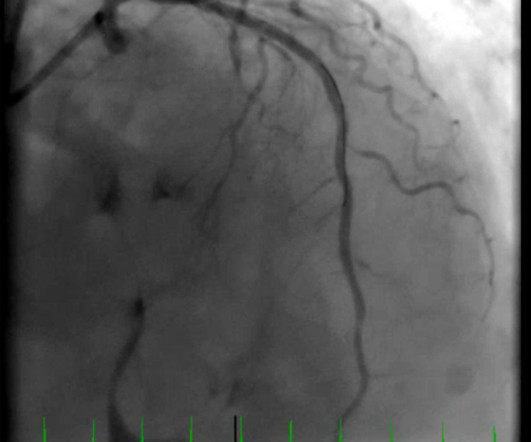
Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. If this patient was managed according to the STEMI/NSTEMI paradigm (although he would be a candidate for early invasive treatment), he would probably be taken to the cath lab hours later. Here is the post-intervention angiogram and post-PCI ECG. 2021.21026.
Here it is: Obvious Inferior Posterior STEMI (+) OMI. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. Aside on ECG Research: 20% of Definite diagnostic STEMI (Cox et al.) The cath lab was activated prehospital But imagine if the patient had walked in.
This patient could have very easily been overlooked, both because the ECG was STEMI negative and because the Q waves were attributed to an “old infarct”. Fortunately, Dr. Cho was not looking for STEMI ECG criteria but for an acute coronary occlusion. OMI or STEMI? As cardiology documented, “possible STEMI.
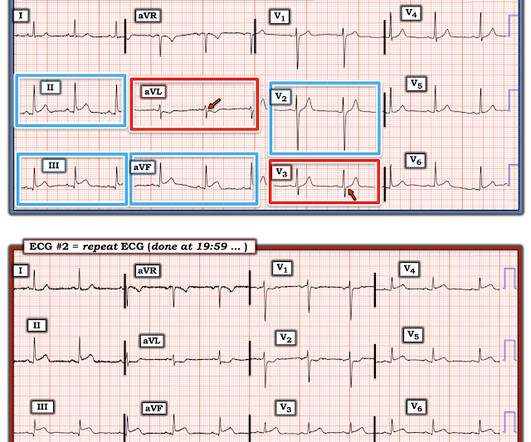
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. They shot this ECG right before going into the ED: Clearly meets STEMI criteria with large STE in V2-V5. Here is the ECG: What do you think?
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later? This caused a type 2 anterior STEMI. The April 8, 2022 post by Drs.
This is my response: "This is definitely acute or subacute. See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. Both support acute anterior STEMI. It is not chronic. There is no question that this benefits from immediate PCI. 3.0 = 0.50
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. 1, 2] The most clinically useful definition to account for this entire constellation is intraventricular conduction delay.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
This is all suggestive of posterior STEMI, but not definitely diagnostic. mm in only one posterior lead is highly sensitive and specific for posterior STEMI). ST depression in V1-V4, isolated, may be either posterior STEMI or NSTEMI. A posterior ECG was done and showed no ST elevation, not even 0.5 Two stents were placed.
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? This is the response he got: Interventionist: "No STEMI, no cath. After stabilizing the patient and recording more ECGs, he tried again: Interventionalist: "It isn't a STEMI." It is a STEMI equivalent. We don't know how many though.
STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. This has resulted in an under-representation of STEMI MINOCA patients in the literature. From Gue at al. Circulation. 2017;135(16):1490–3.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. Sensitivity was 87% for OMI in our validation study (it was 34% for STEMI criteria). Suppose the OMI had been recognized, or suppose another ECG had been recorded and it showed definite OMI.
Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. A millimeter definition of acute STEMI should not be needed to justify the need for prompt cardiac catheterization.
The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Although recognition of OMI was not affected by administration of morphine in this case, use caution with analgesia in ongoing ACS without a definitive plan for angiography. Is there STEMI? Leave it alone. Bigger et al.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
This ECG is highly concerning for LAD occlusion despite it not showing a STEMI criteria. You can find the variables used to calculate the value on MD calc here: [link] Utilizing Dr. Smith’s Subtle Anterior STEMI Calculator (4-Variable), the value is greater than 18.2 which is concerning for LAD occlusion.
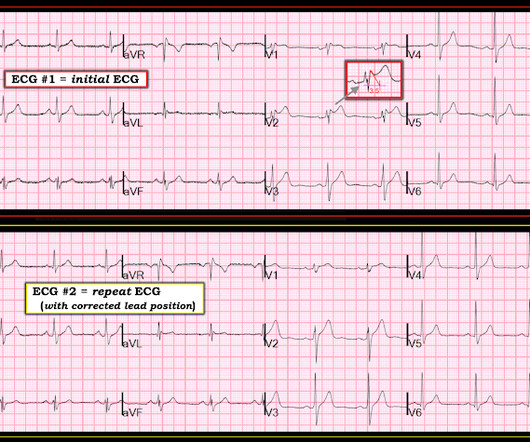
Saddleback ST Elevation is almost never STEMI 2. An inverted P-wave in lead V2 implies lead misplacement too high Saddleback in STEMI: Here are the only 2 ECGs with V2 "saddleback" that I have ever seen which really represented an LAD Occlusion: Anatomy of a Missed LAD Occlusion (classified as a NonSTEMI) A Very Subtle LAD Occlusion.T-wave
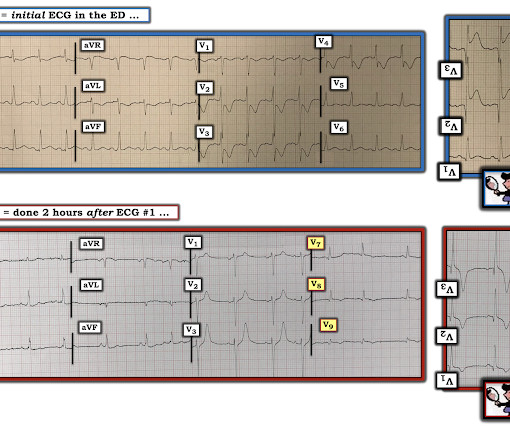
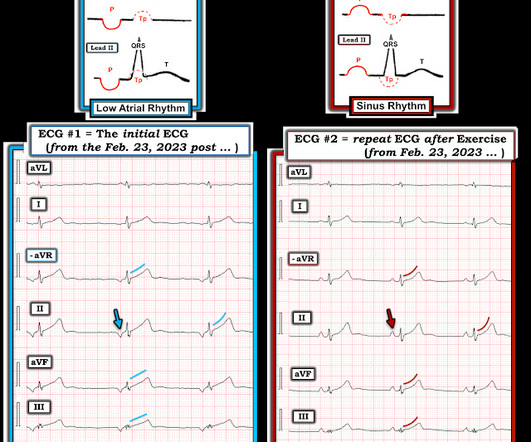
In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. In other words, the inferior "ST elevation" is due to the abnormal rhythm, and does not signify OMI or STEMI in any way. This situation has been named "Emery phenomenon." YOU TOO CAN HAVE THE PM Cardio AI BOT!!
Cardiac arrest #3: ST depression, Is it STEMI? Confirmation of sinus tachycardia should be easy to verify when the heart rate slows a little bit ( as the patient's condition improves ) — allowing clearer definition between the T and P waves. In this case, the cath lab was activated and the patient had a normal angiogram.
There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. However, this STE is definitively abnormal in the setting of a normal QRS complex and hyperacute T-wave morphology in V2. The delay between OMI and STEMI sometimes causes unacceptable loss of myocardium or worse.
He has a history of STEMI and heart failure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. A Coronary angiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. A 50-something had syncope while driving.
This is diagnostic of infero-posterior OMI, but it is falsely negative by STEMI criteria and with falsely negative posterior leads (though they do show mild ST elevation in V4R). They were less likely to have STEMI on ECG, and more likely to be initially diagnosed as non-ACS.
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
Definition: total loss of R-wave means there is a QS-wave (a single deep deflection). He had a prehospital ECG: Obvious anterolateral acute STEMI The patient received aspirin only and his pain immediately resolved: Clear resolution of all ST elevation, with only some residual T-wave inversion in I and aVL. The LAD has reperfused early.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. They are definitely high in amplitude and, intermittently, appear to disproportionately tower over the respective QRS. Closer inspection will show that it is Sinus, after all.
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness. When EMS found her, she was dyspneic and diaphoretic.
In the context of remote rural communities, this can help emergency physicians advocate for their patients, and reduce reperfusion delays by days for STEMI(-)OMI == MY Comment , by K EN G RAUER, MD ( 9/8 /2023 ): == Today’s case is distinguished by its occurrence in a remote rural community ( where the nearest cath lab is a plane ride away ).
This is documented as a STEMI in the clinical notes and in the cath report, but certainly does not meet STEMI criteria and is therefore an NSTEMI by definition. For national registry purposes, this will be incorrectly classified as a STEMI.) Most STEMI have peak cTnI greater than 10.0. ng/mL (ref. < < 0.049).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content