This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
How to document your ultrasound findings. How to document your ultrasound findings. Find us on Patreon here! Buy your merch here! Find us on Patreon here! Buy your merch here!
The post Announcing the National EMS Documentation Survey appeared first on American Ambulance Association. This content is for AAA members only. Please either Log In or Join!
An exploration of clinical documentation and billing/coding with Dr. Robert Oubre (@Dr_Oubre), full-time hospitalist and CDI Medical Director for a community hospital in southern Louisiana. This is based on other diagnoses and factors; hence, document everything. *
Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights Excellent documentation supports standard of care, avoids lawsuit Vertebral artery CVA leaves patient disabled. Result : Based on excellent documentation of thoughtful medical decision making, the case was found to be defensible.
Review the chart (or ask the patient) for prior documentation of intubation or anesthesia to determine if they have a history of a difficult airway. Good practice when documenting: write exactly what you did, and if it was difficult, write why! This can require some interpretation of the context and who was intubating previously.
I dont the exact year these protocols were implemented, but I know that in 2008 they went from a simple typed document to an algorithm format. The document was 222 pages, including 42 medications, 14 procedures, as well as 14 policies. The first document had 170 detailed pages, including 51 medications.
Bryan and Brandon chat about notes: what makes a good one, their many and conflicting purposes, some structures and approaches, system- versus problem-based charting, and more.
University of Maryland Department of Emergency Med
SEPTEMBER 22, 2023
Since the switch from fee for service to value based care in the US, there has been a marked push to improve our documentation to expand ou. Click to view the rest
The ability to import data from the monitor to ESO EHR reduces documentation time while improving the accuracy of your data, allowing you to better focus on the delivery of care. You can use it to directly document and upload FLACC Pain Scores and final score data for non-verbal patients into ESO Insights for easier reporting.
Improvements like longitudinal patient records have transformed episodic documentation into comprehensive patient narratives, aiding both EMS and community health providers in delivering coordinated care. iOS for EHR Coming soon, the new native ESO EHR iOS app is designed to make documenting patient data even easier and more efficient.
That document tells us “Before widespread implementation, CDRs should be compared to clinical judgement.” [3] There is an article published in AEM, with an author list that includes the who’s who of decision rules – from Jeff Kline to Nathan Kupperman to my BFF Chris Carpenter.
Some authors on the ATS document were from Europe, and similarly some authors […] EMCrit Project by Josh Farkas. Within the past year, two major societies have released guidelines on ARDS: the ATS (American Thoracic Society) and the ESICM (European Society of Intensive Care Medicine).
Paramedics increase the current slowly over nearly 3 minutes to 100ma where a documented mechanical capture (pulse palpation site not specified) was noted. Figure 2: Current started at 50 ma without electrical capture, with several native beats signified by the triangle annotated by the cardiac monitor. The ECG strip shown in Figure 3.
It’s an administrative burden that demands extensive documentation and reporting. A modern electronic patient care report (ePCR), like an ESO Electronic Health Record (EHR) , ensures that hospitals can easily capture documentation for standards, such as those required by The Joint Commission.
Dr. Wendy Levinson is the Chair of Choosing Wisely Canada (CWC) and a Professor of Medicine, University of Toronto This SGEM Xtra is based on document created by CADTH and presented at Choosing Wisely Canada […] The post SGEM Xtra: High-Value Care Post Covid19 – Did you ever have to make up your mind?
University of Maryland Department of Emergency Med
NOVEMBER 2, 2023
BACKGROUND: Prehospital (EMS) clinicians are positioned on the front lines of health care. With respect to stroke identification and treatment, ea. Click to view the rest
A draft guidance document was developed after the completion of a national consultation process though an electronic survey with EMTs. Topics were selected by using section titles from the guidance document with a view to seeking further feedback and subsequent refinement of the proposals for CPD. MethodsWillis, et al.
Ciprofloxacin has been documented as a cause of IgA vasculitis. Case Question: What are common triggers for this diagnosis? Common triggers include infection, drugs, and autoimmune. Case Discussion Take-Home Points Consider IgA vasculitis, even in an older patient. References Gamboa F, Rivera JM, Gómez Mateos JM, Gomez-Gras E.
Using a mixed-methods study design, the study consists of three parts: (1) development and implementation of a robust survey tool to identify, quantify, and document the exposure of violent acts committed against paramedics by the public at large, and, by individuals within paramedic service organizations. (2)
What are some of the particulars and caveats surrounding credentialing, documentation, and billing? What are some of the particulars and caveats surrounding credentialing, documentation, and billing? All that and more… We chat about focused, clinician-performed point-of-care ultrasound (POCUS) in the ICU. How do you learn it?
This is also where keeping up with documentation starts to slip. You’ll need to put the following tasks in a rank order list: new patient evaluations, dispositions, managing critical or potentially critical patients, results review, team huddle, running the board, calling consults, doing procedures, and documentation. It’s up to you.
The documentation that is inherent in such a process also facilitates the reporting for performance reviews. Building a defensible and thoughtful set of rules for evaluating responses options in real-time levels the field by providing consistency in the decision-making process.
Photographic documentation of the wound is helpful to enhance continuity of care. Social determinants, such as a history of poor medication compliance, housing insecurity, lack of a support system and transportation resources, comorbidities, or need for vascular intervention, may necessitate inpatient admission.
Current therapeutic guidelines for the management of UTIs in adults First of all, just as a reminder, if you send the urine off for M/C/S for patients who are discharged home, please document under…
The Notice of Funding Opportunity, guidance documents, and other materials are available on the AFG web site. The application period for the FY 2023 Assistance to Firefighters Grant (AFG) is now open. These grants provide funding to fire departments for needed resources such as equipment, gear, vehicles, and training.
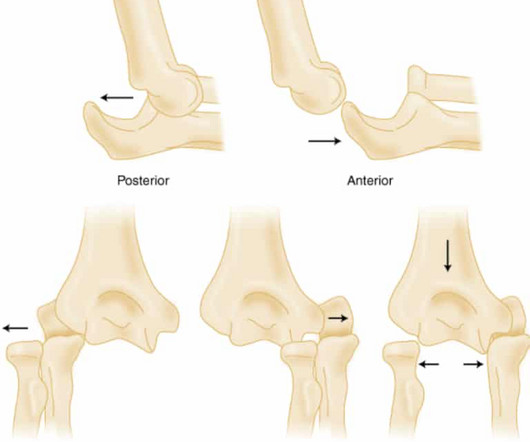
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
The EMR tasks we undertake are expanding rapidly, far beyond simply documenting history and physical examination and every implementation slows us down. There is a long list of things that they do including documentation of the clinical encounter, information retrieval, and discharge preparation.
Fever was documented to be 102°F and was not associated with any chills or rigors. A 40-year-old male, tailor by occupation, was brought to the Emergency Department with complaints of high-grade fever for the past 11 days.
EMS report includes concern for CVA, with variable documentation of face and extremity weakness. Nursing documentation includes the presence of a facial droop. There, his initial neuro exam is documented as normal, but a head CT reveals evidence of a possible acute CVA in the right hemisphere.
.” The tech cleans the wound and documents it as 2cm long and “ dirty.” The ED physician documents suturing a 3 cm laceration in a single layer, omitting any reference to any wound exploration, cleansing or debridement. I thought they were incidental “ bone islands” so I didn ’ t document them. Negligence was present.
We just don’t document it. If we don’t use printed instructions, document our verbal instructions regarding the most common side effects of the drug(s) being prescribed. Documenting our warnings should be standard care. Giving written instructions about a drug is the pharmacist’s job.
Course attendees received an instructor guide, slides, an Emergency Response Guide (ERG), and a resource drive with dozens of forms and documents to assist in local hazmat response planning. Nearly 500 individuals were trained through almost 4,000 contact hours.
13 Interventions may include: Ascertaining a patient’s preferred language early in the clinical encounter (during registration, for instance), and clearly documenting this preference in a place that is visible to all providers. Utilizing certified interpreters and documenting their use. Educating patients on their rights.
In June, we hosted Understanding Accessibility: Practical Strategies for Inclusive Documents, Presentations, and Websites , which provided tips on presenting at conferences that are inclusive to those with disabilities or language barriers.
These “allergies” are often poorly documented and could potentially be more accurately described as intolerance [1]. Background: Penicillin allergies are among the most reported drug allergies, with estimates suggesting that up to 10% of the US population claims to have a penicillin allergy.
There is a well-documented correlation amongst EMS and adult ED physicians who provide less pediatric care to […] The post Pediatric Traumatic Cardiac Arrest appeared first on EMOttawa Blog. Trauma is the leading cause of child and youth mortality globally (1). Pediatric trauma is a high acuity but low frequency event (2).
Frantically look through the assisted care documents for do-not-resuscitate paperwork Place a chest tube on the left side Place a chest tube on the right side Start noninvasive or mechanical ventilation FOR THE RIGHT ANSWER CLICK ON THE ROSH REVIEW LOGO BELOW References: Dixon A. The patient’s emergent portable chest X-ray is shown below.
This integration aims to offer a hybrid solution that respects the preferences of all users, combining the immediacy of digital alerts with the physical presence of sticky notes and faxed documents.
Sponsor Freed is an AI scribe that listens, transcribes, and writes medical documentation for you. It turns clinicians’ patient conversations into accurate documentation – instantly. Due to system constraints, VCU Health Continuing Education cannot offer subscription services at this time but hopes to do so in the future.
We’re defining “protocol” here as a written document that provides oversight from the medical director about how to assess and treat patients. Reassessment and Documentation After any type of restraint is instituted, careful assessment, re-assessment, and documentation is required. Was the documentation complete?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content