This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Triage documented a complaint of left shoulder pain. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." In this version 1, the Queen of Hearts does not compare serial ECGs.
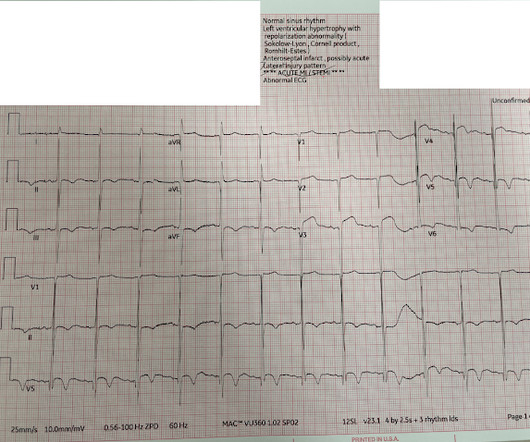
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." found normal ECGs in only 3 of 50 patients with massive PE, and 9 of 40 with submassive PE.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% per year incidence of SCD in this cohort [1].
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Repeat ECG: New developing Q waves in V2 and V3, further confirming evolving OMI.
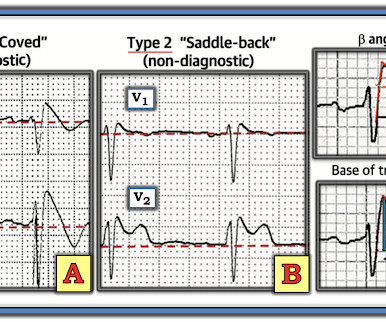
The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. per year incidence of SCD in this cohort [1]. Bicarb 20, Lactate 4.2,
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial.
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Pendell Meyers , Aaron E. I suspect most blog readers did not struggle with this one. Baker , Shifa R.
When I saw this (presented at a conference), I immediately thought it looked like Thype 1 Brugada phenocopy (in other words, Type 1 Brugada ECG pattern ). If the QRS is prolonged, then the differential includes: 1. Criteria for Type 1 Morphology: 1. A flat ST segment will have a Corrado index greater than 1.
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. 1:51, diagnostic RCA angiography At this point, the patient very clearly has a diagnosis of OMI, especially since we visualized embolism within the PDA. & Falk, E. Papadopoulou, E., link] Falk, E., Bossone, E., Galiuto, L.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content