This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
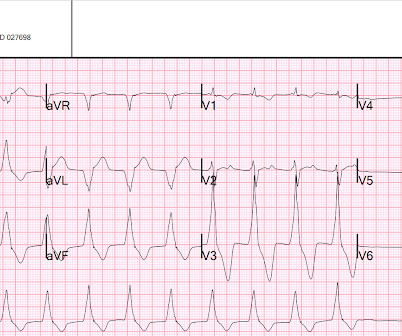
Crew notifies the received ED of an incoming post-arrest patient and notes a sinus bradycardia on their monitor, as seen in Figure 2. The crew increases this current to 75mA and documents an “improvement in patient status” with palpated pulses and a BP of 115/60. Pacing was continued in the ED, with identical settings.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights Excellent documentation supports standard of care, avoids lawsuit Vertebral artery CVA leaves patient disabled.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights The challenge of suicide evaluation in the ED “I’ve changed my mind. If you have a story to share click here.
About three percent of emergency department (ED) visits are due to skin and soft tissue infections, but data are lacking on the contribution of chronic wounds to this number. Wound management in the ED is only a starting point, and appropriate referral and follow-up are key to an improved outcome.
Today’s video evaluates inhaled corticosteroids (ICS) for asthma in the ED setting. EBM Updates: Inhaled Corticosteroids for Asthma in the ED Background : Asthma is a common ED issue, with patient presentations ranging from needing a medication refill to severe exacerbation in respiratory failure.
They were randomized to ceftriaxone 2gm intravenous (IV) in the ambulance or usual cares (fluids and supplementary oxygen) until arrive to the ED. That document tells us “Before widespread implementation, CDRs should be compared to clinical judgement.” [3]
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
This is Bob’s eleventh visit […] The post SGEM#291: Who’s Gonna Drive you to…the ED – with Lights & Sirens? July 2019 Guest Skeptic: Dr. Robert Edmonds is an emergency physician in the US Air Force in Virginia. first appeared on The Skeptics Guide to Emergency Medicine. Date: April 24th, 2020 Reference: Watanabe et al.
Case: It’s another day, another dollar in the emergency department (ED). You wonder if she could have an allergy challenge dose of ceftriaxone in the ED. These “allergies” are often poorly documented and could potentially be more accurately described as intolerance [1]. AEM August 2024. A pivotal study by Raja et al.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Facts : A 24-year-old male is taken to the ED by his parents after “passing out” and being “unconscious for a few seconds.” Defense : The EP did address the seizure when he documented “not post-ictal.”
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Patient not informed of enlarged heart, dies 3 weeks post ED visit Miscommunicated radiology findings are a hot topic. Someone should have – either the first ED doc, the second ED doc, or my PCP.
The EMR tasks we undertake are expanding rapidly, far beyond simply documenting history and physical examination and every implementation slows us down. Research by Hill et al (1) demonstrated that an ED shift can have 4,000 clicks. SGEM#159 looked at the implementation of an EMR in a tertiary care ED.
That includes an episode on steroids to prevent bounce back visits to the ED ( SGEM#28 ), ketorolac for acute treatment ( SGEM#66 ), acupuncture for prophylaxis ( SGEM#211 ) and a calcitonin gene-related peptide antagonist ( SGEM#279 ). Patients with migraines often present to the ED looking for pain relief. Reference: Hartford et al.
AEM January 2021 Case: A 50-year-old male presents to the Emergency Department (ED) with left lower quadrant abdominal pain. That SGEMHOP episode asked how the productivity of APPs compare to emergency physicians and what is its impact on ED operations? There has been a concern about post-graduate training of NPs and PAs in the ED.
Case: You are the medical director of a medium sized urban emergency department (ED). The American College of Emergency Physicians ( ACEP ) has a number of documents discussing APPs in the ED. There has been a concern about post-graduate training of NPs and PAs in the ED. AEM November 2020. AEM November 2020.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. She is seen briefly by the ED physician who orders “ wound cleansing” and an elbow x-ray for “elbow pain.” ” The tech cleans the wound and documents it as 2cm long and “ dirty.”
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. EMS is called, and he is brought to the ED for a reported “slip and fall” with associated facial abrasions. EMS report includes concern for CVA, with variable documentation of face and extremity weakness.
This is also where keeping up with documentation starts to slip. You’ll need to put the following tasks in a rank order list: new patient evaluations, dispositions, managing critical or potentially critical patients, results review, team huddle, running the board, calling consults, doing procedures, and documentation. It’s up to you.
6 24% more likely to return to the ED within 72 hours of their initial visit in an urban ED with >50,000 annual visits. 6 24% more likely to return to the ED within 72 hours of their initial visit in an urban ED with >50,000 annual visits. One cohort study in a public ED found that 84.5%
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. difficile enterocolitis post antibiotic treatment Facts : An adult female presents to the ED with dental pain. We just don’t document it. Documenting our warnings should be standard care.
However, many institutions’ surgical teams still require or request a formal study over a bedside exam, likely due to a lack of confidence in the accuracy of POCUS, resulting in longer ED stays. Moreover, surgeons may seek “official” documentation in a patient’s chart before surgery.
This time the team from Bristol Royal Children’s Hospital ED tell us what is new in the world of paediatric literature… Led by Dr John Coveney a Paediatric Emergency Medicine Trainee in Bristol who has revived The Journal Club at Bristol Royal Children’s Hospital ED on a monthly basis.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. Exam is normal except for tenderness as documented in the diagram. She is diagnosed with “groin pain” and advised to return the next day for US or x-ray if not improved or to go to the ED if worse.
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chest pain that started 2-3 hours earlier while sitting on a porch swing. Here is her ED EKG: What do you think? The physician documented “normal sinus rhythm”. She was successfully defibrillated and taken back to the ED.
Takeaway lessons Many decisions in the ED are less about what to do, and more about when to do it. Takeaway lessons * Many decisions in the ED are less about what to do, and more about when to do it. Goals of care starts in the ED, and not with lip service. ICU time and ED time are different.
A pproximately 65% of these p atients were male , with 63% documented as White non-Hispanic followed by 24% as Black or African American and non-Hispanic. In 2023, EMS clinicians responded to 236,000 calls for suspected opioid overdoses, representing nearly 2% of all EMS calls nationwide.
You are working in a rural ED, and an older woman from a local assisted care facility arrives via ambulance in obvious respiratory distress. EMS is able to tell you that she is currently being treated for pneumonia. The patient is on a nonrebreather mask, and vital signs on arrival are BP 110/50 mm Hg, HR 120 bpm, RR 40/min, T 98.6°F
There is a well-documented correlation amongst EMS and adult ED physicians who provide less pediatric care to […] The post Pediatric Traumatic Cardiac Arrest appeared first on EMOttawa Blog. Pediatric trauma is a high acuity but low frequency event (2).
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. A CBC, Chem 7m and CT of the soft tissues of the neck are ordered by the departing ED doc whose clinical info for the radiologist is “facial swelling”. To opt in to the free subscriber list, click here.
Stevens and colleagues updated their review in 2016 and concluded “sucrose is effective for reducing procedural pain” and “no serious side effects or harms have been documented with this intervention”. That rant relied upon a Cochrane SRMA by Stevens B et al 2013 and a randomized clinical trail published in Pediatrics by Gray L et al 2015.
Here’s another case from Medical Malpractice Insights – Learning from Lawsuits , a monthly email newsletter for ED physicians. He arrives in the ED of his small community hospital about 30 minutes later. The admitting nurse documents an “OTJ injury” with a chief complaint of “My boss made me come.” Updat-ed Jun 23 2021.
In the emergency department (ED), tetracaine drops are applied prior to slit lamp examination and the pain is completely resolved. The first documented use of topical ophthalmologic anesthetics was in 1818. His visual acuity is 20/20 bilaterally and he doesn’t wear corrective lenses or contact lenses.
Using this decision rule would have cut down on ED CT C-spine ordering by >50% in this derivation cohort. I am hopeful it will also improve the flow in the ED.” While plain films for C-spine injury had previously fallen out of routine ED practice, we now have more evidence to support their use in intermediate risk patients.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
We’re defining “protocol” here as a written document that provides oversight from the medical director about how to assess and treat patients. Reassessment and Documentation After any type of restraint is instituted, careful assessment, re-assessment, and documentation is required. Was the documentation complete?
Podcast: Play in new window | Download (Duration: 13:57 — 19.2MB) Subscribe: Apple Podcasts | Google Podcasts | RSS Management of the child with mental health problems who is boarding in the ED In episode 1 of this series, we discussed differentiating organic vs psychiatric causes of agitation in children.
AEM April 2021 * Population: Emergency department (ED) patients 18 years or old where the treating physician determined the need for parenteral sedation for acute agitation (it needed a patient or staff safety concern, not purely a high agitation score). This is an SGEMHOP episode, which means we have the lead author on the show.
I’ve attached an article and an abstract (that article is in Japanese unfortunately … ) that do document that you CAN however on occasion find AIVR in otherwise healthy children — and I suppose that IS what we have here.
While most demonstrations of generative AI applied to the ED involve summarization of records, digital scribing, or composing discharge letters, this attempts clinical decision-support. Likewise, there are other clinical notes of value potentially available, including nursing and triage documentation.
You perform the HINTS exam and the results are reassuring, but the patient’s symptoms persist… Background: Up to 25% of patients presenting to the ED with acute vestibular syndrome (AVS) have a central cause of their vertigo – commonly posterior stroke. You wonder, “Why can’t I just rule out stroke with the HINTS exam?
Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: At the completion of her 1-month elective in your rural emergency department (ED), you are discussing career plans with a medical student. She has worked in five EDs so far, and a man has filled almost every leadership position.
Johnson, MD ( Community EM, Salina Regional Health Center) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF); Marina Boushra, MD (Cleveland Clinic Foundation, EM-CCM); Brit Long, MD (@long_brit) Case A 40-year-old woman presents to a rural emergency department (ED) with left leg pain and swelling for the past 5 days.
This case report documents the first known instance of using NTG during an emergency department resuscitation to treat a patient in cardiac arrest due to severe coronary artery vasospasm. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented. and at Naples Community Hospital in Naples, Fla.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content