This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
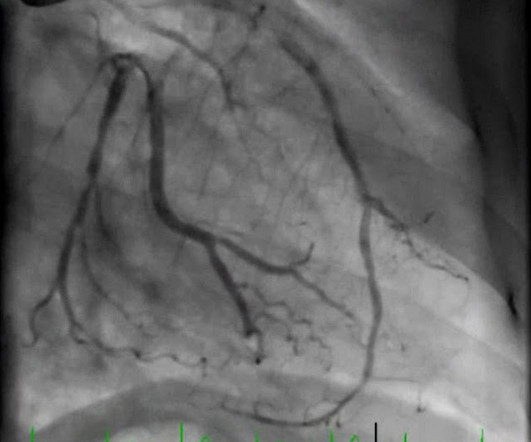
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
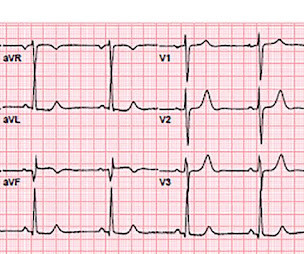
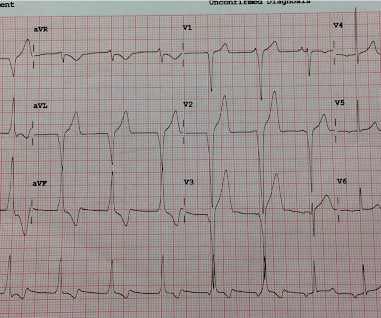
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Click here to sign up for Queen of Hearts Access Case A 58-year-old woman presented to the ED with burning chest pain that started 2-3 hours earlier while sitting on a porch swing. Here is her ED EKG: What do you think? See this post: Septal STEMI with ST elevation in V1 and V4R, and reciprocal ST depression in V5, V6.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
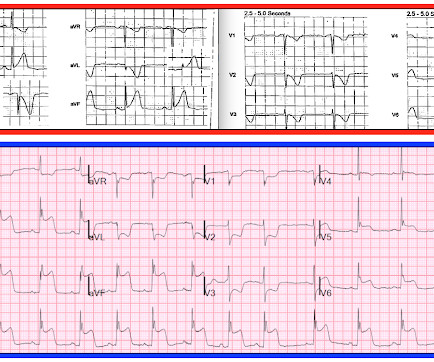
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. The Queen gets it right First ED ECG: Hyperacute T-waves persist.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] have published a number of warnings about the previous reassuring studies.[4,5]
Written by Bobby Nicholson What do you think of this “STEMI”? EKG on arrival to the ED is shown below: What do you think? Second, although there is a lot of ST Elevation which meets STEMI criteria, especially in V3-4, the ST segment is extremely upwardly concave with very large J-waves (J-point notching). or basilar ischemia.
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
The Queen of Hearts agrees: Here the Queen explains why: However, it was not interpreted correctly by the providers: ED interpretation of ECG: "paced rhythm, LBBB but no STEMI pattern." Most large STEMI have peak troponin I in the 20.0 Next trop in AM. Peak trop 257.97 Smith: This is an enormous myocardial infarction.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Triage documented a complaint of left shoulder pain. Immediate versus delayed invasive intervention for non-stemi patients. She contacted her neighbor, a nurse, for help. The case continues.
Gender, race, ethnicity, and socioeconomic disparities are well-documented within the healthcare system. One of these areas is assessing patients with ED-diagnosed strokes. While stroke assessment is documented 38% of the time for patients overall, it is only documented 32% of the time for Hispanic/Latino patients.
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). He appeared to be in shock.
Ongoing pain noted throughout all documentation, but after nitro drip and prn morphine, "pain improved to 2/10." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Setting – large, academic, suburban ED. CT aorta negative for dissection.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." The RR ( R espiratory R ate ) in today's case is recorded as 14/minute at the time the patient presented to the ED on the day after their initial presentation. Today's Initial ECG: As per Drs.
It was worse on the evening prior to presentation while lying in bed, then recurred and resolved while at rest just prior to arriving in the ED. Here is the first ED ECG, with no pain: Sinus rhythm. New ST elevation diagnostic of STEMI [equation value = 25.3 Computerized QTc = 419. Computerized QTc = 417. Heart 1996;75:222–228.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS.
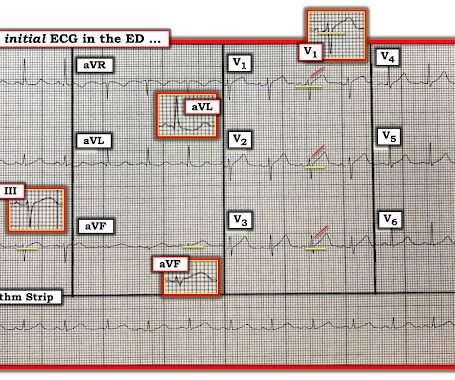
He still had active pain on arrival to the ED. This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. His initial ECG in the ED ( = E CG # 1 ) is shown in Figure-1.
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergency department (ED). The patient initially presented to an outside ED and was subsequently transferred to our facility for continuity of care.
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. His HEAR score (before troponin resulted) was documented at 3, with documentation stating "low suspicion for ACS."
They gave him 2 nitroglycerine and transported to the ED. In the ED, the patient was "moaning, writhing in bed, and clutching his chest." Here is the first ED ECG (there was no previous ECG on file for comparison): Sinus rhythm and LVH There is some (less than 1 mm) of STD in V3 and V4. It was not a STEMI) 1.
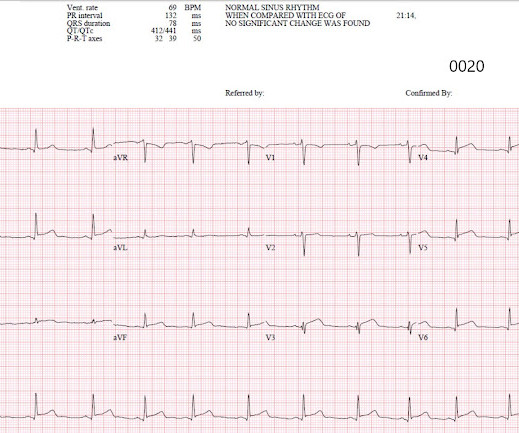
Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Learning Points: This is one of many examples of false positive STEMI criteria, which is distinguishable by expert humans, and now by AI such as QOH. No prior ECG was available.
This is of course diagnostic of an acute coronary occlusion MI (OMI) that also meets STEMI criteria. Then this was recorded in the ED 10 minutes after the first: Now there is massive STE Many inferior MI are associated with RV MI. BOTTOM — 2nd ECG obtained 10 minutes later in the ED ( See text ). Can you tell from this ECG?
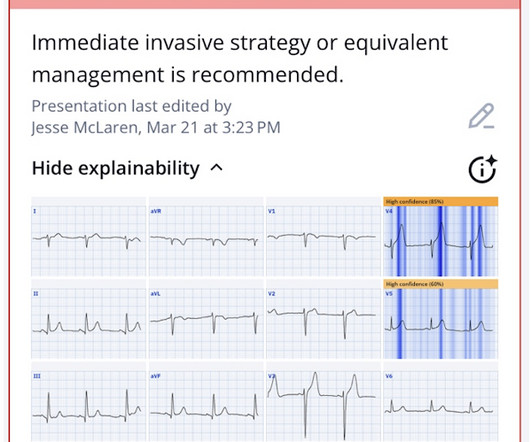
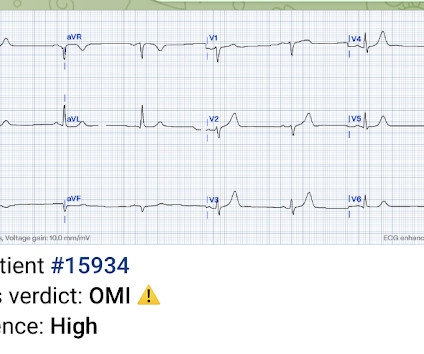
This was marked as "Not a STEMI" by the physicians. It is not a STEMI, but it is diagnostic of an LAD OMI (Occlusion MI). has outperformed many cardiologists in its ability to recognize with "high confidence" acute OMIs from ECGs not satisfying STEMI-criteria. This was sent to me by a friend.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. He denied chest pain or shortness of breath.
A 40-something woman presented to the ED having had “heartburn” overnight and then worsening chest pain 1 hour prior to arrival. Here is the ED ECG (no previous ECG was available for comparison). T his is a systematic failure that has been documented in the following study: Garg A, Lehmann MH. The patient looked ill.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
Of course, the bill for any episode of emergency department (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices. Now, many acute pyelonephritis patients receive an IV antibiotic, analgesia, and an antiemetic in the ED. This process required at least a full day.
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chest pain described as an “explosion" of left chest pressure. At the time of arrival to the ED, the patient reported 1/10 chest pain with normal vital signs. Triage EKG: What do you think? 1] Wereski, R.,
He wrote in his note that "The EKG showed early repolarization in I, V2-V3 but no clear STEMI pattern." We performed a beside US (shown below) which showed lateral wall hypokinesis as read by an US-boarded ED attending in real time. See far below for data on 24 troponin T in STEMI and NSTEMI, and correlation with infarct size.
The patient was diagnosed with a"Non-STEMI." Traditionally , Occlusion MI (OMI) myocardial infarctions that are not STEMI are called NonSTEMI. That said — we do know that ECG #2 was the last ECG on file prior to this patient’s presentation to the ED on the day of admission. To me, that is a meaningless diagnosis.
I’ve attached an article and an abstract (that article is in Japanese unfortunately … ) that do document that you CAN however on occasion find AIVR in otherwise healthy children — and I suppose that IS what we have here. Is there STEMI? Most physicians, at first glance, get this wrong. What is it? What is the rhythm? Giant R-waves.
A middle-aged man presented with 7-8/10 non-radiating chest tightness to the left chest wall, associated with nausea but no diaphoresis, that began while walking approximately 40 minutes prior to arrival at the ED. He was definitely pain free by the time of arrival at his ED room. What do you think? Chest Pain scores can be misleading.
Sent by Anonymous, written by Pendell Meyers A man in his 60s with history of CAD and 2 prior stents presented to the ED complaining of acute heavy substernal chest pain that began while eating breakfast about an hour ago, and had been persistent since then, despite EMS administering aspirin and nitroglycerin.
A prehospital ECG was recorded (not shown and not seen by me) which was worrisome for STEMI. Here was his initial ED ECG: There is sinus tachycardia at a rate of about 140 There is profound ST Elevation across all precordial leads, as well as I and aVL. A near 60 year old male called 911 for increasingly severe fever and SOB.
How would YOU interpret ECG #1 if this was the only tracing you saw — and — the only thing you knew about the patient, was that he/she was being seen in the ED? At this point — I learned a bit more about today's patient: The patient is a man who had an inferior STEMI in 2010. He presented to the ED for today's visit because of vertigo.
This is a re-posting of a Tweet by Robert Jones (@RJonesSonoEM), reproduced with permission, written by Pendell Meyers A middle aged female with history of smoking presented to the ED with "bad heartburn." Here is her prior baseline ECG (first), and her ED ECG (second): Baseline: ED ECG: What do you think?
This is why it is essential that the OMI/NOMI paradigm replace the STEMI/NonSTEMI paradigm. Under Non-STEMI, this patient would not have intervention until at least 20 hours (next day), after the infarct is completed. Learning Points: 1. 25-30% of OMI are not treated in a timely way.
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5
2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. Cardiology was consulted and they agreed that the EKG had an atypical morphology for STEMI and did not activate the cath lab. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. Bicarb 20, Lactate 4.2,
The medicine note documents that the patient had worsening pain with lying flat and relief with leaning forward. Myocarditis is virtually indistinguishable in the ED from MI. See this case: Pericarditis, or Anterior STEMI? I n the intervening 3 hours, new Q-waves have developed in leads V3 and V4, and deepened in V5 and V6.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
Thus, Brugada is the likely diagnosis _ A very nice explanation of this is given in the document quoted below on current ECG criteria for Brugada pattern. If there are any syncopal or presyncopal events, she should be evaluated immediately in the ED. --All Bayes de Luna, A et al. All 1st degree relatives should have 1 time EGG.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content