This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
All of the secondary outcomes (mortality at 90 days, misdiagnoses, hospital length of stay, ICU admission rate, ICU length of stay, and quality of life) also did not show a statistical difference between the intervention group and the control group (SGEM#207).
We chat about focused, clinician-performed point-of-care ultrasound (POCUS) in the ICU. What are some of the particulars and caveats surrounding credentialing, documentation, and billing? All that and more… We chat about focused, clinician-performed point-of-care ultrasound (POCUS) in the ICU. How do you learn it?
These “allergies” are often poorly documented and could potentially be more accurately described as intolerance [1]. The use of direct oral challenges has been tried in the intensive care unit (ICU) setting to de-label patients.
Yes, temporize with supportive care while you go through the process, but do the work—find a legitimate representative or documentation of the patient’s wishes to determine what they’d want before you commit them to lengthy, aggressive life support. ICU time and ED time are different. Emergency staff have limited bandwidth.
Population 18+-year-old patients admitted with septic shock to a Medical ICU in an academic hospital in Mexico. Length of ICU stay: 1.5 This paper thoroughly documents patient assessments, vasopressor titration protocols, and methylene blue dosing. sodium chloride over 6 hrs once daily for 3 days. p<0.001. hrs p<0.001.
ClinicalTrials.gov: NCT02517489 7 Clinical Question: In adult patients with severe community-acquired pneumonia admitted to the ICU, does early hydrocortisone treatment, compared to standard therapy, reduce mortality at 28 days? ICU-acquired infections were observed in: 9.8% Patients enrolled from 31 Intensive Care Units in France.
Exam is normal except for tenderness as documented in the diagram. She admitted to the ICU for “DKA.” She never had a documented abdominal exam. I just failed to document it. The EP documented seeing the patient and agreed with the ARNP’s plan. If you take a history or examine a body part, document it.
What They Did: Double-blind, randomized, placebo controlled trial that ran from October 2019 through January 2024 Multinational study conducted at 22 centers in three European countries 3512 patients were enrolled and before surgery eligible patients were randomly assigned to one of the following two groups Amino Acid Group: 10% Isopuramin at a dose (..)
Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. Kuttab et al’s findings, constituting 45% of the review’s weight, suggest that administering <30cc/kg IVF is associated with increased odds of mortality, delayed hypotension, and increased ICU utilization. 2.89, p = 0.01.
Blood Component Timing: It was documented that 76% of patients requiring PRBCs received them within four hours of arriving at the hospital. This is a significant increase from last year’s findings, where just 46% of qualifying trauma patients received PRBC within four hours of arrival.
She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. She had an uneventful ICU course and was extubated for ongoing care with the inpatient psychiatric service.
The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Human Errors and Adverse Hemodynamic Events Related to “Push Dose Pressors” in the Emergency Department. J Med Toxicol. Epub 2019 Jul 3. PMID: 31270748 Maheshwari K, et al. Intensive Care Med. 2018;44(6):857–67.
2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. 2019 Aug; PMID: 30954692 Clinical Question: What is the impact of system factors in the implementation of standard-of-care LPV in critically ill ED patients admitted to the ICU? Paper: Owyang CG, et al.
Propofol utilized for sedation; patient admitted to ICU for EEG monitoring. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents. While second attempt ongoing, neck prepped and marked for cric. Second attempt with DL and bougie successful; ETT position confirmed with US.
The patient was upgraded to the ICU for closer monitoring. I cannot tell you how many times such "written" documentation was off, due to the tendency to inscribe a normal number instead of counting for 30 seconds because "the patient looked like they were breathing normally".
The TEG group had a shorter ICU length of stay in the first admission. Patients exclusively managed in the ICU which decreases applicability for patients in other locations Very small sample size of 96 patients No definition was provided for exclusion criteria of significant cardiopulmonary disease.
Diagnosis and management of infections with this bug are a common occurence in the ICU and it behoves us to have a working knowledge of some of the complexities of its investigation and treatment that often fall to our micro or ID colleagues. The next job is to document clearance from the blood.
Digestive Management Takeaway: Start enteral feeds when the patient gets to the ICU. Statements: Initiate EN as soon as possible after ICU admission (100%, 20/20). These conversations should occur frequently and be clearly documented for other health care professionals who are not present during the conversations (96%, 22/23).
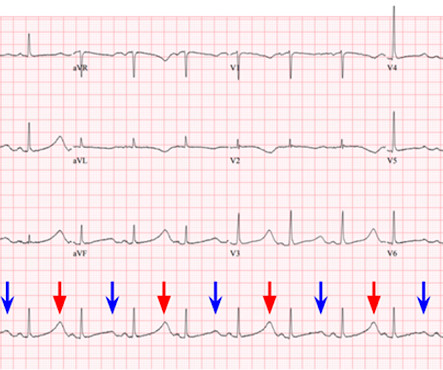
Source: [link] As you are calling the ICU and cardiology team, the patient has recurrence of her symptoms and repeat ECG shows return of the PVT. The literature base for the use of lidocaine for torsade storm is documented primarily by case studies in drug-induced TdP. Another ECG is obtained and shown below. Adapted from wikipedia.
This segues relatively nicely into a section of the document on palliative care. It is important to realise that a referral to ICU for refractory cardiorenal syndrome may simply be a sign that the patient is reaching end of life.
Intensivists have embraced the tracheostomy as an ICU procedure. There is a substantial ANZICS document on tracheostomy that forms the structure for this tasty morsel. In a breaking from what could only loosely be described as tradition at this point, this podcast is going to be in 2 parts.
The pacing rate was increased without clinical improvement and the patient was transferred to the ICU for closer monitoring/treatment. A bed side echocardiography revealed a severely depressed LVEF of about 20-25%. When looking at the above ECG you will find that the QRS following ventricular pacing is very long.
. * the hyperaemic phase: about a quarter will have this at around day 3-7 and it seems ill defined but it’s suggestive you can lower your MAP targets here a bit Overall the basic bundle of interventions in the ICU for ICP include: * sedation – this is needed for the tube but also it reduces metabolic rate considerably and reduces ICP.
Consequences of this are well documented and include delayed treatment, exposure to error, increased length of stay, and increased mortality. Emergency departments (EDs) provide the essential service of evaluating patients with unscheduled, acute, undifferentiated, and decompensated conditions. ED crowding impairs this mission.
Other times, present AI may simply fall short of a human’s ability to identify a net new diagnosis that is not based on existing documented knowledge, or is currently classified as “idiopathic.” Finally, AI algorithms require large amounts of data to be accurate and reliable, which can be difficult to obtain in some cases.
This has relevance to the ICU population in 2 major ares * Sepsis. * EF does not correlate with particularly well with mortality in sepsis though diastolic dysfunction does * It may be due to under filling and the reduced diastolic filling due to the ubiquitous tachycardia in sepsis.
ABG and VBG Correlation The correlation between venous and arterial blood gases is well-documented for standard differences (Table 1), and the data obtained from the VBG can be acted on as if it were an ABG (1, 3-6). Importantly, the comparison between an ABG and VBG is site-specific, as illustrated below (Table 1) (1, 3-6).
Thiamine also plays a role in key metabolic processes, including cellular energy production and generation of cellular antioxidants, and thiamine deficiency has been well-documented in sepsis, with observational studies indicating a signal for improved outcomes with supplementation. The primary outcome was hospital survival.
Reliance on Electronic Health Records Data : As with many retrospective studies, reliance on EHR data for identifying eligible patients and outcomes is prone to inaccuracies, missing data, and variability in clinical documentation practices. Comorbidity Index : Higher in the cefepime group (median 2 vs. 1). vs. 52.2%). Pettigrew et.
They should be admitted to hospital in case of clinical deterioration to receive ICU treatment. However, there are documented adverse events such as haemorrhagic cerebrovascular accidents or recurrence of VOC after drug withdrawal, which represent a drawback in its regular use. This treatment is usually done in the ICU setting.
Executive Summary: International Clinical Practice Guidelines for Pediatric Ventilator Liberation, A Pediatric Acute Lung Injury and Sepsis Investigators (PALISI) Network Document. Implementation of a Risk-Stratified Opioid and Benzodiazepine Weaning Protocol in a Pediatric Cardiac ICU. Am J Respir Crit Care Med. 2023;207(1):17-28.
This document will focus on the anatomical considerations and aspiration risk. It is true, someone finally did an RTC on ICU level patients and found that first pass success IS better with VL than DL (Prekker 2023), but the fact remains that sometimes VL fails. fiber optic through the nose).
4,5 Of particular concern is the Sudanese conflict, which began in April 2023, and which has caused the largest internal displacement of a population in documented history. 84 All patients with severe malaria need inpatient admission, ideally to the intensive care unit (ICU). Severe malaria is typically caused by P.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content