This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The post Announcing the National EMS Documentation Survey appeared first on American Ambulance Association. This content is for AAA members only. Please either Log In or Join!
Review the chart (or ask the patient) for prior documentation of intubation or anesthesia to determine if they have a history of a difficult airway. Good practice when documenting: write exactly what you did, and if it was difficult, write why! Find us on Patreon here! Buy your merch here! Find us on Patreon here! Buy your merch here!
An exploration of clinical documentation and billing/coding with Dr. Robert Oubre (@Dr_Oubre), full-time hospitalist and CDI Medical Director for a community hospital in southern Louisiana. This is based on other diagnoses and factors; hence, document everything. * Requiring additional monitoring is also contributory.
Chuck Pilcher, MD, FACEP Editor, Medical Malpractice Insights Editor, Med Mal Insights Excellent documentation supports standard of care, avoids lawsuit Vertebral artery CVA leaves patient disabled. Result : Based on excellent documentation of thoughtful medical decision making, the case was found to be defensible.
I dont the exact year these protocols were implemented, but I know that in 2008 they went from a simple typed document to an algorithm format. The document was 222 pages, including 42 medications, 14 procedures, as well as 14 policies. The first document had 170 detailed pages, including 51 medications.
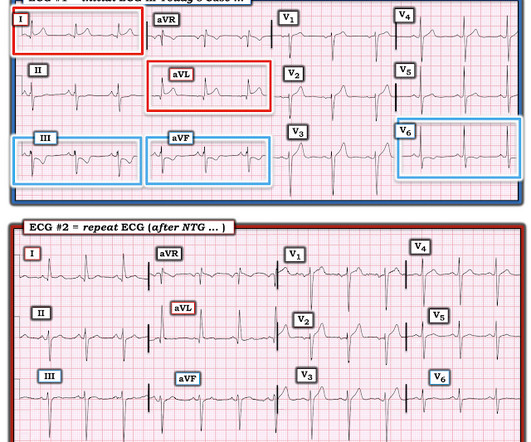
Chest Pain – Benign Early Repol or OMI? Written by Destiny Folk, MD, Adam Engberg, MD, and Vitaliy Belyshev MD A man in his early 60s with a past medical history of hypertension, type 2 diabetes, obesity, and hyperlipidemia presented to the emergency department for evaluation of chest pain. But — Which ST-T wave is the "correct" one? (
The crew increases this current to 75mA and documents an “improvement in patient status” with palpated pulses and a BP of 115/60. As seen in Figure 4, the current is higher, the phantom complexes are larger, but they do not have true electrical capture. Figure 4 : Pacer set to 60 mA with false electrical capture and native beats.
Cardiology consult note written around that time documents that "Pain improved with NTG, morphine in ED but still present." Smith comment: But the tests (ECG and troponin) are extremely specific and so the post test probability is nearly 100%. Repeat cTnI drawn at around 8 AM was 3.910 ng/mL. This patient was not one of the lucky 6.4%
That document tells us “Before widespread implementation, CDRs should be compared to clinical judgement.” [3] A randomized control trial (RCT) done in the prehospital setting enrolled 2,698 patients. However, getting the right diagnosis is clearly important for our patients, and as good as we are, no clinician is perfect.
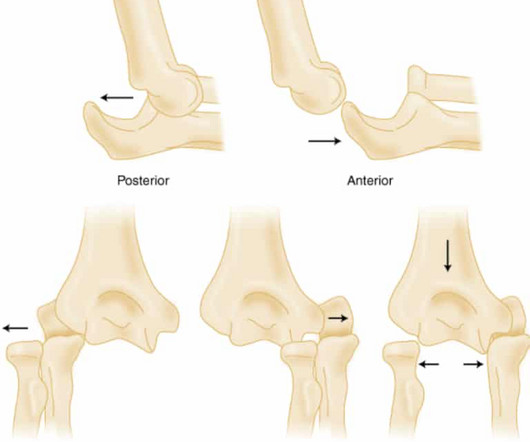
Elbow Dislocation Definition: Disarticulation of the proximal radius & ulna bones from the humerus Epidemiology: Incidence Second most common joint dislocation (after shoulder) in adults Most commonly dislocated joint in children Accounts for 10-25% of all injuries to the elbow ( Cohen 1998 ) Posterolateral is the most common type of dislocation (..)
The ability to import data from the monitor to ESO EHR reduces documentation time while improving the accuracy of your data, allowing you to better focus on the delivery of care. You can use it to directly document and upload FLACC Pain Scores and final score data for non-verbal patients into ESO Insights for easier reporting.
We documented that the majority of stenotic lesions had compensatory enlargement and thus exhibited remodeling. Strictly speaking — this case does not at this time qualify as MINOCA — because the negative cath and 2 normal hs-troponins done 6 hours apart failed to document infarction. (
And you can see why: the artery may sponstaneously reperfuse, as it did here well before angiography, and documented with resolution of pain and evolution of the ECG to typical full reperfusion pattern Peak troponin I was 8544 ng/L. This is diagnostic of full reperfusion.] 90% of normals have some STE in V2 and V3. Which 1 or 2 leads are KEY?
Poorly healing wounds are primarily the result of chronic venous insufficiency, peripheral (arterial) vascular disease, prolonged pressure-point skin injury, or neuropathy secondary to vascular disease or diabetes. Once identified, they must protect the skin from further injury. Examples include Adaptic, Xeroform, Telfa, and Dermagen.
While the list is not exhaustive an d critical incidents can vary from person to person, their documentation is crucial for protecting your own team and further improving research for the entire industry. Documenting exposure to critical incidents is key. So, what else can your organization do?
Ciprofloxacin has been documented as a cause of IgA vasculitis. The patient stated that she was started on Cipro eyedrops 1 or 2 days prior to presentation for a possible eye infection. It was not on her palms or soles. She had no mucous membrane involvement. They are somewhat raised, non-blanching, not itchy, and non-tender.
Improvements like longitudinal patient records have transformed episodic documentation into comprehensive patient narratives, aiding both EMS and community health providers in delivering coordinated care. iOS for EHR Coming soon, the new native ESO EHR iOS app is designed to make documenting patient data even easier and more efficient.
The documentation that is inherent in such a process also facilitates the reporting for performance reviews. Emergency medical care in the field should not be simply the first rung of a ladder to other health care careers, but a profession where providers can earn a living wage commensurate with the hazards of the care they afford to others.
Paramedics increase the current slowly over nearly 3 minutes to 100ma where a documented mechanical capture (pulse palpation site not specified) was noted. He has a past medical history of HTN, HLD, DM, seizures, and ESRD with a regular hemodialysis schedule (per family, he adheres to his schedule meticulously).
A critical MORSEL is that every child you treat for DKA needs to have an initial thorough neuro exam including cranial nerves and then frequent neuro reassessments … and document it ( so your colleagues who take over care for the kid can know if there has been a change )! or serum bicarbonate between 5-10 mmol/ L Severe : venous pH < 7.1
It’s an administrative burden that demands extensive documentation and reporting. A modern electronic patient care report (ePCR), like an ESO Electronic Health Record (EHR) , ensures that hospitals can easily capture documentation for standards, such as those required by The Joint Commission.
This is also where keeping up with documentation starts to slip. You’ll need to put the following tasks in a rank order list: new patient evaluations, dispositions, managing critical or potentially critical patients, results review, team huddle, running the board, calling consults, doing procedures, and documentation.
The nurse completes the Columbia-Suicide Severity Rating Scale (C-SSRS) and documents that the patient’s recent thoughts of killing himself and his detailed plan makes him “High Risk” for suicide. There is no documented handoff to the on-coming emergency physician (EP) who assumes care. ” 0700 : The PA-C goes off-shift.
One of the first documented strikes among house staff officers took place in 1974 at Howard University here in Washington, D.C., Historically, labor unionization among health care workers is uncommon, 5 including among resident physicians, 6 and the prospect of striking even more so. This victory is about more than just numbers.
Exam documents that he is alert and oriented but “tired appearing” and “not appearing post-ictal.” Defense : The EP did address the seizure when he documented “not post-ictal.” There is no negligence, as the documentation supports reasonable judgment. The triage nurse records the event as a “seizure” lasting 7 minutes.
Fever was documented to be 102°F and was not associated with any chills or rigors. A 40-year-old male, tailor by occupation, was brought to the Emergency Department with complaints of high-grade fever for the past 11 days. Case Question: What clinical condition is associated with eschars?
A draft guidance document was developed after the completion of a national consultation process though an electronic survey with EMTs. A draft guidance document was developed after the completion of a national consultation process though an electronic survey with EMTs. Qualitative analyses were performed using NVivo (version 10).
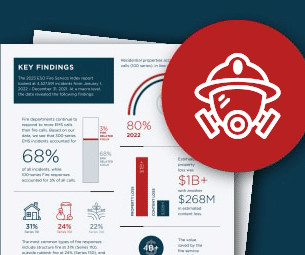
According to a recent study from ESO , decontamination procedures were only documented in 82% of all working fires incidents, and out of those exposures, only 4% documented all on-scene decontamination procedures. This leaves significant of room for improvement. What can the industry do?
The amazing part of this story is that it took more than 20 years for the scientific community to prove this theory to be correct and for other doctors to accept it as standard practice. This interesting piece of history defines the term neophobia, or the fear of something new. Are there are evolutionary reasons for neophobia?
These “allergies” are often poorly documented and could potentially be more accurately described as intolerance [1]. Background: Penicillin allergies are among the most reported drug allergies, with estimates suggesting that up to 10% of the US population claims to have a penicillin allergy. A pivotal study by Raja et al.
EMS report includes concern for CVA, with variable documentation of face and extremity weakness. EMS report includes concern for CVA, with variable documentation of face and extremity weakness. Nursing documentation includes the presence of a facial droop. He is transported to a different hospital as possible trauma.
In June, we hosted Understanding Accessibility: Practical Strategies for Inclusive Documents, Presentations, and Websites , which provided tips on presenting at conferences that are inclusive to those with disabilities or language barriers.
An unknown EP reviews the report, determines that there is no reason to notify the patient, and documents nothing. It wasn’t, so you weren’t called, nor did the doc need to document anything. This patient’s history was either poorly taken or poorly documented. Too much weight was given to the EKG, CXR, and labs.
13 Interventions may include: Ascertaining a patient’s preferred language early in the clinical encounter (during registration, for instance), and clearly documenting this preference in a place that is visible to all providers. Utilizing certified interpreters and documenting their use. Educating patients on their rights.
Course attendees received an instructor guide, slides, an Emergency Response Guide (ERG), and a resource drive with dozens of forms and documents to assist in local hazmat response planning. Pipeline and Hazardous Materials Safety Administration. This is the NVFC’s second SPST grant.
Exam is normal except for tenderness as documented in the diagram. She never had a documented abdominal exam. I just failed to document it. The EP documented seeing the patient and agreed with the ARNP’s plan. There is no mention of an abdominal exam. She is given 60 mg IM ketorolac for thigh pain. It was benign.
We just don’t document it. If we don’t use printed instructions, document our verbal instructions regarding the most common side effects of the drug(s) being prescribed. Documenting our warnings should be standard care. Complications result in a total colectomy with its accompanying lifestyle changes. difficile colitis.
In Australia, for example, AHPRA’s Paramedicine Board describes paramedics as "practitioners" throughout documentation regarding registration. As paramedics, whilst we often take great offence at being called ambulance drivers, the question is, when it’s our turn to drive, what exactly is it that we are providing?
Stevens and colleagues updated their review in 2016 and concluded “sucrose is effective for reducing procedural pain” and “no serious side effects or harms have been documented with this intervention”. That rant relied upon a Cochrane SRMA by Stevens B et al 2013 and a randomized clinical trail published in Pediatrics by Gray L et al 2015.
.” The tech cleans the wound and documents it as 2cm long and “ dirty.” The ED physician documents suturing a 3 cm laceration in a single layer, omitting any reference to any wound exploration, cleansing or debridement. I thought they were incidental “ bone islands” so I didn ’ t document them. I just didn ’ t document it.
The American College of Emergency Physicians ( ACEP ) also has a number of documents discussing APPs in the ED. AEM January 2021 Case: A 50-year-old male presents to the Emergency Department (ED) with left lower quadrant abdominal pain. The patient is seen by an advanced practice provider (APP).
It seems like just yesterday ( or maybe ~ a month ago ) when we served up a tasty morsel on the PECARN decision rule for intra-abdominal traumatic injuries in children. Our friends at the PECARN injury group have remained busy this spring with generating more externally validated clinical decision rules. High Risk (12.8% High Risk (12.8%
All cases with restraints should be clearly documented, in some systems medical control should be involved, QA of all these cases should be considered. Article Summary by Sarah Fabiano, MD, FACEP, FAAEM Kupas DF, Wydro GC, Tan DK, Kamin R, Harrell AJ 4th, Wang A. Prehosp Emerg Care 2021 Sep-Oct;25(5):721-3. doi: 10.1080/10903127.2021.1917736.
We’re defining “protocol” here as a written document that provides oversight from the medical director about how to assess and treat patients. Protocols Every EMS agency should have protocols for dealing with agitated or violent patients. Sometimes these can also be referred to as guidelines, standing orders, policies, or procedures.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content