This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Negative E-FAST and no signs of long bone injuries should raise concern for neurogenic shock in the hypotensive trauma patient with suspected spinal injury. Alpha 1 agonists are necessary to maintain appropriate blood pressure. Both norepinephrine and epinephrine can be used. Tenenbein M, Macias CG, Sharieff GQ, et al, eds.
Sinha 2012] It is useful in the prehospital setting , correlating well with actual weight and ED Broselow weight. Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh.
1-5] Since then, many more medications have been developed and deployed. These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. 1] CV manifestations include: Bradycardia, tachycardia, ventricular dysrhythmias, cardiac arrest. [1-5]
to 1 case per 100,000 children. 2][3] Bacterial tracheitis should be suspected over croup if nebulized racemic epinephrine or steroids do not improve the clinical course. [2][3][8] 2][3] Bacterial tracheitis should be suspected over croup if nebulized racemic epinephrine or steroids do not improve the clinical course. [2][3][8]
Features Urticaria and pruritis Rapid onset (1-2 hours) IgE Dependent (Type I Hypersensitivity) Reactions An allergen cross-links two or more IgE molecules on mast cells or basophils and initiates a signal cascade leading to degranulation. J Allergy Clin Immune Tract 2017; 5(5): 1402-9. In: UptoDate, Feldweg AM (ed.)
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
Patients were randomized in a 1:1 ratio. Key Secondary Endpoints: 5 (3.9%) patients in the IV cetirizine group returned to any ED or clinic within 24 hours compared to 15 (11.1%) in the IV diphenhydramine group; P=0.04 A contraindication, known allergy, or suspected intolerability to the study medication.
Vittinghoff, E. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. The prohibition against beta blockade in cocaine toxicity, causing "unopposed alpha" stimulation, needs to be re-examined. is intuitive, and not surprising.
When simple maneuvers fail, we proceed to topical agents such as lidocaine with epinephrine, oxymetazoline, anterior nasal packing, and electrical or chemical cauterization. TXA has become the standard practice in the ED based on small RCTs, though larger trials have not demonstrated the same benefit ( REBEL EM review ).
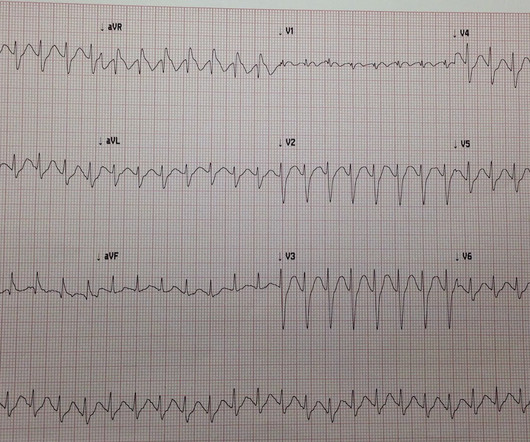
On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. At about 30 minutes after presentation, the patient had acceptable vital signs with the TVP and low dose epinephrine drip. Another ECG was obtained during pacing: Mostly paced rhythm with PVCs (#3, #6, #9, #12). mm STE with 9.5
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. or 9 size endotracheal tube to allow for bronchoscopy and/or endobronchial blocker placement whenever necessary. These patients are at imminent risk of respiratory failure.
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. He underwent CPR, and regained a pulse after epinephrine, with an organized narrow complex rhythm at 140, but still with severe shock. Here they are: Learning Points: 1. He was moderately hypoxic.
On arrival to the ED, her blood pressure is 84/36 mmHg with a heart rate of 110 beats per minute. 3,4 Prompt recognition and management of sepsis and septic shock are paramount for the ED clinician. This was based on studies that demonstrated qSOFA was more specific but less sensitive than its counterparts (Table 1).
1 In addition to intentional overdoses, there are multiple case studies of abuse (ingestion, insufflation, injection). QRS > 100 msec can give sodium bicarbonate 1-2 mEq/kg IV boluses. 9-12 Do not use this prophylactically in bupropion overdoses. Other Norepinephrine or epinephrine are preferred vasopressors when needed.
You will find the list is broken down into four sections: 1.Reviews Arch Dis Child Fetal Neonatal Ed. 2024 Apr 9. Arch Dis Child Fetal Neonatal Ed. Associations of excessive internet use, sleep duration and physical activity with school absences: a cross-sectional, population-based study of adolescents in years 8 and 9.
A 67-year-old man presents to the emergency department (ED) in cardiac arrest. Multiple attempts at defibrillation, epinephrine, and amiodarone have been unsuccessful. On ED presentation, he is unresponsive and the monitor shows ventricular fibrillation. 2018;13(9):e0204169. Margey R, Browne L, Murphy E, et al.
She describes the pain as left-sided, non-radiating, and 9/10 in severity. Answer: Takotsubo Cardiomyopathy 1-18 Background: Also known as transient apical ballooning syndrome, apical ballooning cardiomyopathy, stress-induced cardiomyopathy, stress cardiomyopathy, Gebrochenes-Herz syndrome, and broken-heart syndrome.
A 43-year-old male with a history of mitral valve regurgitation s/p valvular replacement, hypertension, hyperlipidemia was evaluated in the ED for septic shock secondary to a pyelonephritis with a renal abscess. Chu CK, Delia E, Mograder A, Dwyer EM. 2017;45(1):12-20. 2015;7(9):E365-E369. J Saudi Hear Assoc. J Thorac Dis.
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. Resuscitated with chest compressions, epinephrine. including epinephrine, and there was ROSC. Not a shockable rhythm. Resuscitation was begun with chest compressions, etc.,
In the ED, he develops recurrent respiratory depression and hypoxia to 80%. 1 Most heroin in the United States actually contains fentanyl and fentanyl analogs. Naloxone reverses the analgesic, respiratory, sedative , and miotic e ffects of opioids. 6 Image 1: Structure of naloxone. How long should they stay in the ED?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content