This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Due in large part to the proliferation of anonymous chemical factories able to produce industrial volumes of inexpensive synthetic opioids without opium or other controlled precursors, fentanyl spilled into the United States, Canada, and Europe, heroin soon fell to market forces [1, 2]. Some patients require re-dosing in the ED.
Pathophysiology Primary injury happens at the time of the traumatic event or shortly after in the high cervical to mid-thoracic spine. Negative E-FAST and no signs of long bone injuries should raise concern for neurogenic shock in the hypotensive trauma patient with suspected spinal injury. 2011;46(9):1771. 5 th Edition.
In many emergency departments (ED), US machines are readily available and can be used to rapidly assess and monitor patients with acute dyspnea at the bedside. What They Did: Design: Randomized, controlled, blinded-outcome trial Sites: Three emergency departments in Denmark Duration: October 9, 2019 to May 26, 2021.
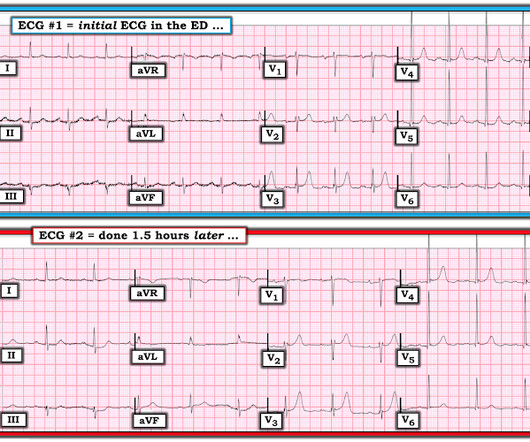
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
I agree, however: 1) I don't think you can get a good enough ech o without bubble contrast. 3) E cho is another step that takes time. I had only 9 false positives but I missed 2 OMI. The rhythm for the ECG in Figure-1 is sinus — with normal intervals and axis ( mean QRS axis about +80 degrees ). Time is myocardium.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. Learning Point: 1. For examples of such exceptions — See My Comment in the January 9, 2019 — August 22, 2020 — and June 30, 2023 posts in Dr. Smith's ECG Blog ).
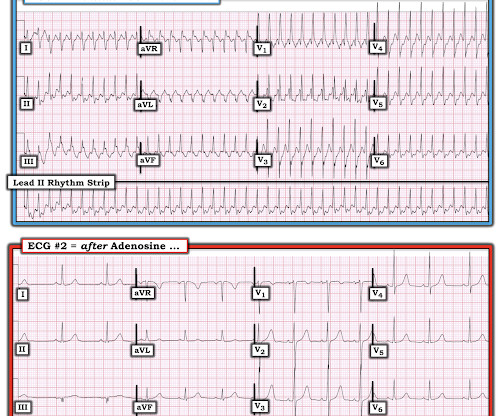
Clinical Question: Does simultaneously performing the modified valsalva maneuver and administering intravenous adenosine, compared to either treatment alone, have greater success in achieving normal sinus rhythm in patients presenting to the ED with PSVT? Duration of Antiarrhythmic Effect: MVM group: 35.44 seconds (range: 22.5,
The parents of 9-month-old Josie bring her into the Emergency Department with coryzal symptoms and difficulty breathing. Among those who do not always obtain a CXR, one-fifth still routinely obtained them under a certain age (2 weeks to 12 years, median of 1 year). doi: 10.1590/s1516-31802007000300005 Beyyumi, E., AlDhanhani, H.,
A 58-year-old female with a history of diabetes, hypertension, and chronic back pain presents to the ED with severe headache and nausea. Answer : Pneumocephalus 1-21 Background: Pneumocephalus is defined by the presence of air within the cranial cavity. Pain control and antipyretics Strict avoidance of Valsalva maneuvers (i.e.,
1-5] Since then, many more medications have been developed and deployed. These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. 1] CV manifestations include: Bradycardia, tachycardia, ventricular dysrhythmias, cardiac arrest. [1-5]
1 Prehospital endotracheal intubation and EGAs are typically placed without paralytics and are reserved for unconscious, apneic, and out-of-hospital cardiac arrest patients. 9 LMAs use an inflatable mask expanded using a similar technique to the endotracheal tube cuff. In: Cone DC, Brice JH, Delbridge TR, Myers B, eds.
A 74-year-old female with a past medical history of hypertension, diabetes, recent basilar artery stent placement with a 20 pack-year smoking history presents to the ED via EMS for altered mental status and episodes of apnea. CT head without contrast 1 is performed and reveals the following: Question: What is the diagnosis?
” – Musings of an American ED resident in July 2022 when US healthcare was affected simultaneously by supply chain issues from GE Healthcare (contrast media) and Abbott Laboratories (Similac baby formula). 3 A study of CT use trends in the ED has shown increasing use of CTs by almost 60% from 2005 to 2013. 11 Table 1.
Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5. We can, therefore, put down the defibrillation pads, set aside the amiodarone, and look further at the ECG.
The Importance of Civility in Critical Care Resuscitation A 3-year-old patient with diabetic ketoacidosis arrives at your ED. Once a sufficiently high level is achieved, modelling of behaviours and episodes of retaliation can perpetuate the behaviours far beyond the initial event. Here are ten things to think about: 1.
[link] Case continued She arrived in the ED and here is the first ED ECG. IMPRESSION: 1. We know that most type 1 acute MI due to plaque rupture and thrombosis occurs in lesions that are less than 50% (see Libby reference). I don't know if her pain was getting better or not. The Queen no longer thinks it is OMI.
Features Urticaria and pruritis Rapid onset (1-2 hours) IgE Dependent (Type I Hypersensitivity) Reactions An allergen cross-links two or more IgE molecules on mast cells or basophils and initiates a signal cascade leading to degranulation. J Allergy Clin Immune Tract 2017; 5(5): 1402-9. In: UptoDate, Feldweg AM (ed.)
A 37-year-old G2P2 female with no other past medical history presents to the ED with a 2-day history of intermittent fever and foul-smelling vaginal discharge. Therefore, these antibiotics would not be appropriate in the event that the patient had pelvic inflammatory disease or endometritis secondary to chlamydia or gonorrhea.
Background: Atrial fibrillation and atrial flutter with rapid ventricular rate (AF/AFL with RVR) are the most common subtypes of SVT, comprising a large number of ED visits in aging populations. Investigators enrollend 660 patients in 9 years in 5 EDs; or approximately 6 patients per month; or 1 patient per /month for each ED.
Patients were randomized in a 1:1 ratio. Key Secondary Endpoints: 5 (3.9%) patients in the IV cetirizine group returned to any ED or clinic within 24 hours compared to 15 (11.1%) in the IV diphenhydramine group; P=0.04 The effectiveness of IV cetirizine was determined to be statistically non-inferior.
Article 1: Positive urine cultures without pyuria Wang ME, Jones VG, Kane M, et al. Clinical Course of Children 1 to 24 Months Old With Positive Urine Cultures Without Pyuria. 2024;24(1):111-118. Arch Dis Child Fetal Neonatal Ed. Giannoni, E., Acad Pediatr. doi:10.1016/j.acap.2023.06.023 Epub ahead of print.
A 77-year-old man presented to the emergency department (ED) with hip pain following a fall. On ED presentation, he was experiencing 10 out of 10 pain level. A radiograph is shown (see figure 1). LEARN MORE The most common nerve blocks in this study are shown in Table 1. 2023 Sep 2;15(9):e44583. J Patient Saf.
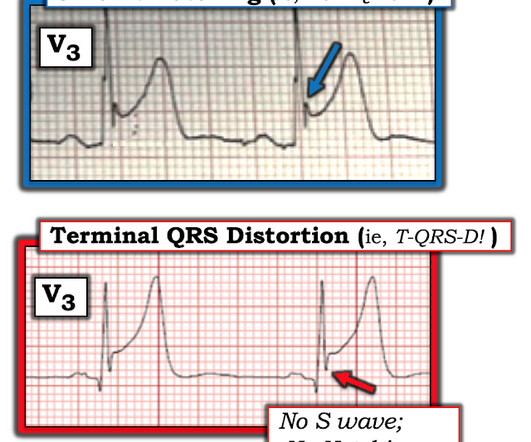
I’ve taken th e l ead V 3 examples in Figure-1 from previous cases posted on Dr. Smith’s ECG Blog : T OP in Figure-1 — Despite marked ST elevation in this lead V3 — this is not T-QRS-D, because there is well-defined J-point notching ( BLUE arrow ). This patient had a repolarization variant as the reason for ST elevation.
PSA, also referred to as intravenous sedation in this paper, requires considerable resources, including 1:1 nursing observation, and burdens the emergency department (ED). 1.01, I2 = 69%, low certainty) Fewer adverse events occurred in the IAL group compared to the PSA group. vs. 91.4%; RR 0.93; 95% CI 0.86–1.01,
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. ECG’s can be labeled as ‘normal’ by the computer (and confirmed by cardiology) even with diagnostic signs of occlusion or reperfusion References 1. JAMA Intern Med 2019 9. Am J Med [Internet] 2017;130(9):1076–83.e1.
You will find the list is broken down into four sections: 1.Reviews Arch Dis Child Fetal Neonatal Ed. 2024 Apr 9. Arch Dis Child Fetal Neonatal Ed. Associations of excessive internet use, sleep duration and physical activity with school absences: a cross-sectional, population-based study of adolescents in years 8 and 9.
Fill Your Social Calendar at ACEP23 Beyond the 200 educational courses, the ACEP23 lineup also includes fun social events every night. If you’d like to grow your professional network while you’re in Philly, these events could be a great opportunity to meet new people. Learn more at acep.org/acep23/social.
On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. Another ECG was obtained during pacing: Mostly paced rhythm with PVCs (#3, #6, #9, #12). The ED team again pointed out the evidence of inferoposterior OMI, this time by the modified Sgarbossa criteria. mm STE with 9.5 mm STE with 9.5
Introduction Pediatric intubations in the emergency department (ED) occur at only a tenth the frequency of adult intubations. 1 Pediatric rapid sequence intubation (RSI) in the ED is associated with a higher frequency of failed first attempts and adverse effects than in adult patients. mg/kg IV, ketamine at 1.5–2 3 mg/kg IV.
References: 1) See this study showing an association between morphine and mortality in Non-STE-ACS: Meine TJ, Roe M, Chen A, Patel M, Washam J, Ohman E, Peacock W, Pollack C, Gibler W, Peterson E. Setting – large, academic, suburban ED. Figure-1: The initial ECG in today's case.
A 3-year-old male was brought to the emergency department (ED) by his mother, who reported the sudden onset of a rash (hives) covering his entire body, with no rash on his palms and soles. FIGURE 1: Abdominal X-ray showing particulate radiopaque foreign bodies involving the stool. 1 Children are particularly vulnerable.
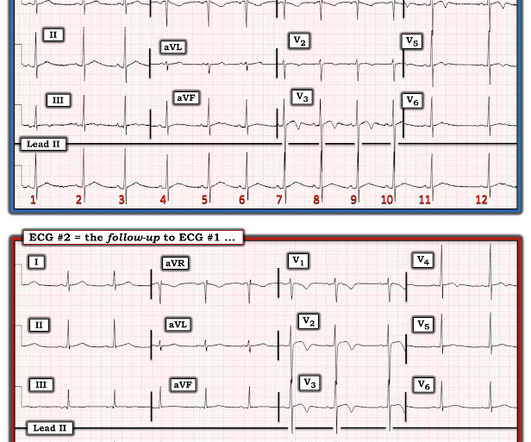
. == MY Comment by K EN G RAUER, MD ( 9/27/2019 ): == As suggested by the title of this Blog post — confirmation of the diagnosis in this case was made not by ECG — but instead by chest aorta CT ! For clarity — I’ve put these first 2 tracings together in Figure-1. Figure-1: The first 2 ECGs in this case ( See text ).
Queen: #1: NOT OMI, HIGH CONFIDENCE Queen: #2: NOT OMI, HIGH CONFIDENCE ECG 1 Interpretation: there is terminal T-wave in V3-V6. LEARNING POINT : 1. For clarity in Figure-1 — I've reproduced and put together the 2 serial ECGs that were texted to Dr. Smith in today's case. in ECG #1 ). Smith: Young thin black male.
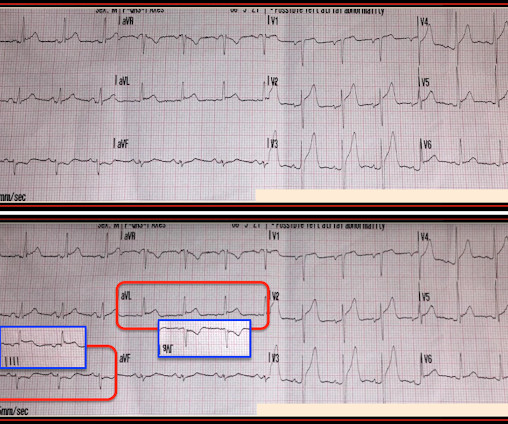
For clarity — I’ve put these 2 tracings together in Figure-1. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). The ECG finding that I KNOW is real in ECG #1 is the mirror - image appearance of ST-T waves in leads III and aVL.
Patients were randomly assigned 1:1 to treatment with either an ambulatory device or standard guideline-based management (aspiration, standard chest tube insertion, or both). Patients were observed for 1-2 hours for clinical stability, and placement was confirmed with a chest x-ray.
TXA has become the standard practice in the ED based on small RCTs, though larger trials have not demonstrated the same benefit ( REBEL EM review ). 2013 Sep;31(9):1389-92. Adverse Effects: No serious adverse events were noted. However, the benefit vs. harm of using TXA topically for epistaxis is unclear. Am J Emerg Med.
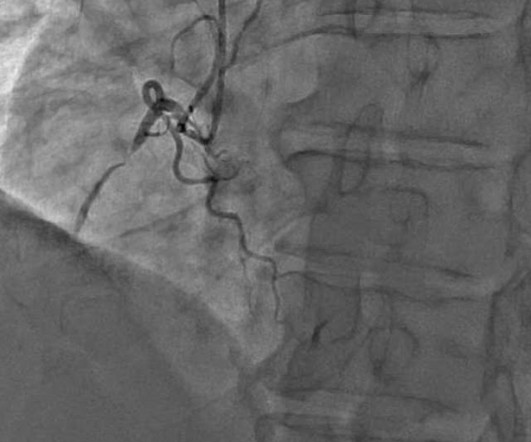
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Proven STEMI has an open artery in 19% to 36% of cases, depending on whether it is TIMI −1, −2, or −3 flow. 25] Stone et al found that 72% have TIMI 0 or 1 flow.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chest pain and shortness of breath after finishing a 4-mile run. At the time of evaluation in the ED, his symptoms were resolved. He typically runs 4 to 8 miles per day.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Takotsubo is a sudden event, not one with crescendo angina. Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
It's important and useful to note that 1) Over 90% of healthy young men have up to 3mm ST elevation in one or more precordial leads normally (Atlas of Electrocardiography by K. My Comment , by K EN G RAUER, MD ( 8/9/2018 ): == Our thanks to Lou B for this insightful case. But there is clear ST elevation in lead aVL in Figure-1.
A 30-something was in the ED for some minor trauma when he was noted to have a fast heart rate. See Learning point 1 below. mg/kg IV is administered if no response is seen and no significant drug-induced adverse event occurs. They usually lasted anywhere between 1-2 hours. He acknowledged that he had palpitations.
I found a well appearing young lady in the room with her parents who witnessed the event. She denied having any symptoms before or after the event, and she was asymptomatic on my initial exam. The ED catheter was removed at that point and she did not require any further procedures. She was discharged home in good condition.
The patient arrived in the ED. The pain completely resolved after nitroglycerine Moments later, the this ECG was recorded in the ED when she had been pain free for moments only: Computer read: Normal ECG. If you use something like the HEART score: 1. E EKG: a negative ECG (score = 0) 3. Learning Points : 1.
TXA has been mentioned previously on PEM Morsels in the following contexts: Post Tonsillectomy Hemorrhage , Hemophilia in the ED , Von Willebrand Disease , Epistaxis in Children , Hereditary Angioedema , Hemoptysis in Children , Hyphema , and even in Neonatal Subgaleal Hemorrhage. 2012 Feb;147(2):113-9. Acad Emerg Med.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content