This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What is the next step in evaluation and treatment? fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
1 While PJP gained significant recognition among HIV-positive adults during the early AIDS epidemic, the growing utilization of immunosuppressants has resulted in an increased incidence of the disease in individuals who are HIV-negative. 9 The signs and symptoms of PJP infection are non-specific. for detecting pulmonary opacities.
In a surprise to no one who reads First10EM, clinical judgment is better than all decision tools for sepsis Knack SKS, Scott N, Driver BE, Prekker ME, Black LP, Hopson C, Maruggi E, Kaus O, Tordsen W, Puskarich MA. Epub 2024 Apr 9. 2024 Mar;27(1):26-29. 2024 Jul 4;391(1):9-20. doi: 10.1016/S0140-6736(24)00700-1.
1-5] Since then, many more medications have been developed and deployed. These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. 1] CV manifestations include: Bradycardia, tachycardia, ventricular dysrhythmias, cardiac arrest. [1-5]
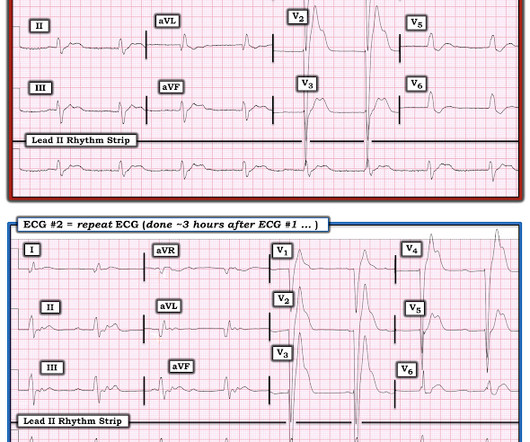
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. C Examination notable for diaphoresis, 1+ bilateral lower extremity edema, regular heart rate and rhythm, and no signs of respiratory distress with normal breath sounds. The patient was upgraded to the ICU for closer monitoring.
He has already climbed Ben Nevis in Scotland, visited the Gobi desert (possibly from the comfort of his parents 4 x 4, but who’s judging) and has his bronze D of E nailed. All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. A PEM Adventure Ranulf is a 14-year-old explorer.
A 65 y/o Female was admitted to the ICU for septic shock. Question 1: What is the rhythm? Beat 1 : Sinus, narrow QRS complex. The assumption is that a premature complex discharged prior to Beat 1, which prolonged its respective refractory period in the same manner as Beat 5.
to 1 case per 100,000 children. 2][3][9] Hypoxia, respiratory muscle retractions, fatigue, altered mental status, and decreased breath sounds are signs indicative of impending airway failure. [2] 2][3][9] Glucocorticoid were not shown to alter clinical course or patient outcomes. [2][3] 2017;7(1):16-23. Rev Infect Dis.
Do we need to intubate French drunkards in ED? 2013 Sep;24(9):1848-53. 2023 Nov 28;27(1):465. 2024 Apr 1:e240167. 2023 Sep 8;9(1):73. 117(1) 36–41 DOI: 10.1177/01410768231207260 This is a fascinating read about the history of the humble placebo in science. Psychol Sci. doi: 10.1177/0956797613479386.
A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. 1 Risk Factors: 1-4 Spontaneous Anticoagulants (Apixaban, Rivaroxaban, etc.)
PMID: 34890894 Myth 1: Kayexalate is safe and useful. 2024 Jan 2;53(1):afad255. Yerke JR, Mireles-Cabodevila E, Chen AY, Bass SN, Reddy AJ, Bauer SR, Kokoczka L, Dugar S, Moghekar A. Casey wrote a protocol for peripheral noradrenaline 9 years ago… in 2015! Am J Emerg Med. 2022 Feb;52:85-91. doi: 10.1016/j.ajem.2021.11.030.
The Importance of Civility in Critical Care Resuscitation A 3-year-old patient with diabetic ketoacidosis arrives at your ED. The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. Here are ten things to think about: 1. 2014 Jun 26;23(12):653-9. 2020 Jan 1;35(1):70-6.
You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergent management? The median age at diagnosis was 47 months (range 1-173 months). 2014;9(9):S102-S109. Arch Dis Child Educ Pract Ed.
mg/dL (sorry, Europeans, for the weird units) Here was the initial ED ECG: There is a junctional rhythm with retrograde P-waves (see the dip in the T-wave in lead II across the bottom; you can follow that up to all the other leads and see the retrograde P wave). He was admitted to the ICU and was unstable, in shock, overnight.
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. in the ICU but survived with excellent function. 15-9/6/2017 ). Figure-1: Excerpt from ESC review on acute pericarditis ( See text ).
You, however, are working an ED shift, and when you see the name “Barbie Junior” on your computer screen, your heart does a flutter. It can be in started in the ED, and many of us are already using it. Secondary outcome analysis showed there was no difference in length of hospital stay, ICU stay, or duration of oxygen therapy.
Paper: Smith JA, Secombe P, Aromataris E. 95% Confidence Interval) Strengths: The study addresses a patient-centered clinical question that is relevant to ED practice. 95% Confidence Interval) Strengths: The study addresses a patient-centered clinical question that is relevant to ED practice. J Trauma Acute Care Surg.
1 The American College of Surgeons’ (ACS) Trauma Quality Improvement Program (TQIP) Massive Transfusion in Trauma Guidelines leave a good amount of flexibility for hospitals regarding transfusion protocols, focusing more on systems-level aspects of designing and implementing MTPs.2,3 in the 1:1:1 group vs. 17.0%
One of the most hair-raising presentations to the emergency department (ED) can be massive hemoptysis with respiratory failure. or 9 size endotracheal tube to allow for bronchoscopy and/or endobronchial blocker placement whenever necessary. These patients are at imminent risk of respiratory failure.
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. On arrival in the ED, he was hypotensive with a systolic blood pressure in the 70s. What is it?
Due in large part to the proliferation of anonymous chemical factories able to produce industrial volumes of inexpensive synthetic opioids without opium or other controlled precursors, fentanyl spilled into the United States, Canada, and Europe, heroin soon fell to market forces [1, 2]. Some patients require re-dosing in the ED.
As the only respiratory therapist in the ED has been paged and is starting BiPAP for this patient, an overhead call for two incoming trauma alerts from a multivehicle collision sounds. Importantly, the comparison between an ABG and VBG is site-specific, as illustrated below (Table 1) (1, 3-6).
On arrival to the ED, her blood pressure is 84/36 mmHg with a heart rate of 110 beats per minute. 3,4 Prompt recognition and management of sepsis and septic shock are paramount for the ED clinician. This was based on studies that demonstrated qSOFA was more specific but less sensitive than its counterparts (Table 1).
A 64-year-old male presents by EMS to the ED with shortness of breath. 1 There are over 50,000 visits related to heart transplant in the United States each year and over half of these patients are admitted to the hospital from the ED. We’ll keep it short, while you keep that EM brain sharp.
An 8-year old male with a history of sickle cell anemia presents to the ED for evaluation of fever for 2 days and “feeling like I can’t get a full breath”. 2 mcg/kg, max 100 mcg) while obtaining IV access 20 IV/IM ketorolac (1 mg/kg, max 15 mg) Morphine (05-0.1 C or 100.4 mg/kg, max 4 mg per dose q20-30min) or hydromorphone (0.01-0.02
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. 1-5 Farmers also treat sheep for parasites using OPs and may become symptomatic after exposure, an illness called Dipper’s Flu.
What They Did: Investigators performed a retrospective cohort study in the Emergency Department at the University of Michigan between July 1, 2014 through December 31, 2018. Imbalances Between Treatment Groups : ICU Admissions : Higher in piperacillin-tazobactam (33% vs. 30%). 9 Instrumental Variable Analysis? vs. 52.2%).
Figure 1: Clinical manifestations and long-term consequences of sickle cell disease Training and education on sickle cell disease: Training and education are crucial to improve morbidity and mortality. with thanks A 15-month-old Kenyan boy presents to ED with right hand swelling. Blood culture is pending.
A 43-year-old male with a history of mitral valve regurgitation s/p valvular replacement, hypertension, hyperlipidemia was evaluated in the ED for septic shock secondary to a pyelonephritis with a renal abscess. Left ventricular outflow tract obstruction in ICU patients. Chu CK, Delia E, Mograder A, Dwyer EM. 2017;45(1):12-20.
A 65-year-old male with a past medical history of chronic obstructive pulmonary disease on 2 liters per minute (LPM) nasal cannula at baseline, hypertension, hyperlipidemia, and polypectomy presents to the ED with 2 days of worsening shortness of breath, pleuritic chest pain, persistent fevers, and productive coughs with occasional hemoptysis.
On arrival to the ED the patient’s initial vital signs are temperature 38.5C, BP 102/48, HR 106, RR 20. 1 The incidence of iron overdose and iron ingestion related deaths has significantly decreased over time, likely attributable to federal regulation. 1 Table 1: Iron content of various preparations.
While this guide isnt exhaustive, its designed by residents, for residents, to provide practical tips and foundational knowledge thats crucial in the fast-paced, high-stakes environment of the ED. Introduction Airway management is a critical ED skill to master. Just the uvula but not the pillars, class 2.
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 g/dL, thrombocytopenia of 96 10 9 /L, prothrombin time (PT) of 16.1 1 By the end of 2023, 117.3 of the global population.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




























Let's personalize your content