This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
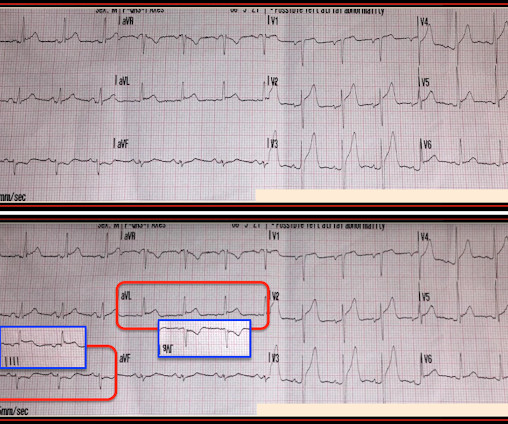
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI."
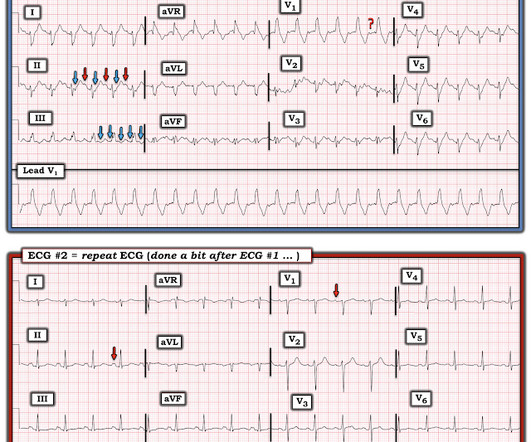
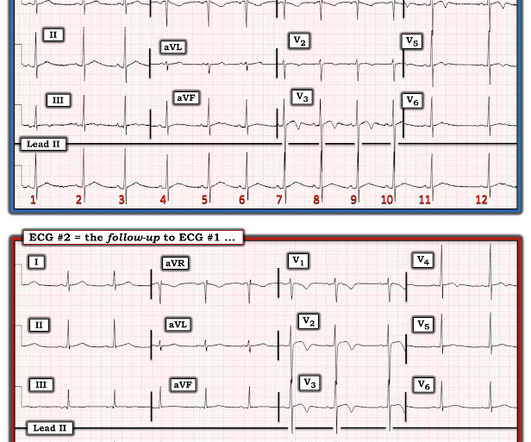
The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Here is lead I from ECGs 1 and 2 shown side-by-side to highlight the change in axis from borderline right to completely normal. Her ECG is shown below: What do you think?
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
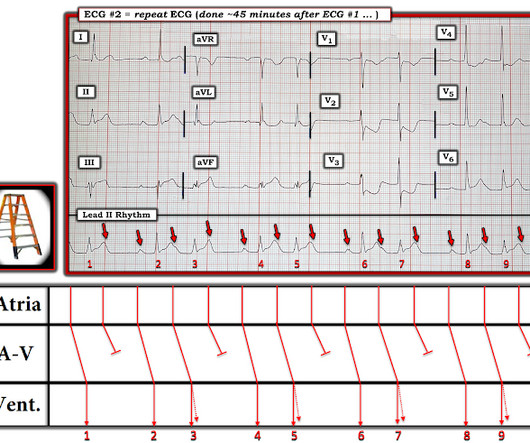
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case. After seeing ECG #2 — Can you explain: i ) Why no negative P wave was seen in lead V1 of ECG #1? —
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." found normal ECGs in only 3 of 50 patients with massive PE, and 9 of 40 with submassive PE.
[link] Case continued She arrived in the ED and here is the first ED ECG. IMPRESSION: 1. We know that most type 1 acute MI due to plaque rupture and thrombosis occurs in lesions that are less than 50% (see Libby reference). I don't know if her pain was getting better or not. The Queen no longer thinks it is OMI.
An ECG was performed in the ED at 1554: Original image unavailable, this is the only recorded scanned ECG available. A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. per year incidence of SCD in this cohort [1].
Furthermore, the term "STEMI equivalent" has no reliable or definable meaning except between two practitioners who both agree on the list of entities that they believe are STEMI equivalents and can agree on how to identify it. Obvious inferoposterior STEMI. J ACC 61(4):e78-140; page e83.
He had walked into the ED (did not use EMS). Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. J Am Coll Cardiol 53(17):1503-9. Plum mer D, Dick C, Ruiz E, Clinton J, Brunette D.
A 40-something with persistent Ventricular Fibrillation presented after attempted prehospital resuscitation A 40-something with no previous cardiac history presented to the ED in persistent Ventricular Fibrillation after attempted prehospital resuscitation. Figure-1: The initial ECG in today's case — obtained after ROSC.
He had walked into the ED (did not use EMS). Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Lessons : 1. Exact pain history was difficult to ascertain.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. Setting – large, academic, suburban ED.
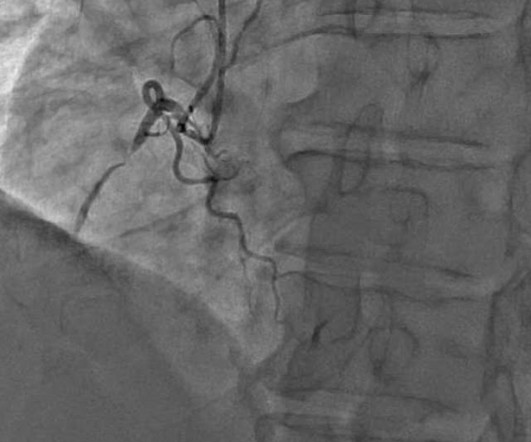
Here is his ED ECG: There is bradycardia with a junctional escape. There is an obvious inferior posterior STEMI(+) OMI. We recorded an ECG in which V1-V3 were put in the position of V4R-V6R, and V4-6 were placed in V7-9 to (academically) confirm posterior OMI. Atropine usually works in junctional rhythm with a narrow complex 9.
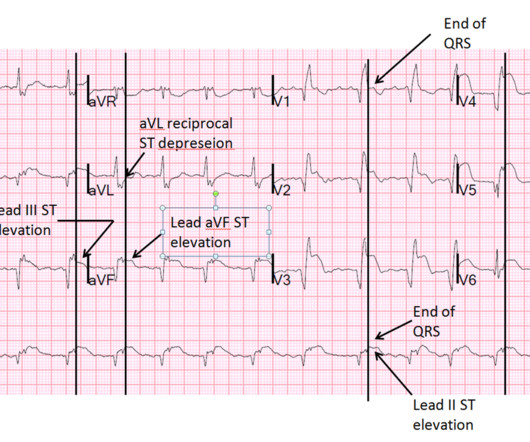
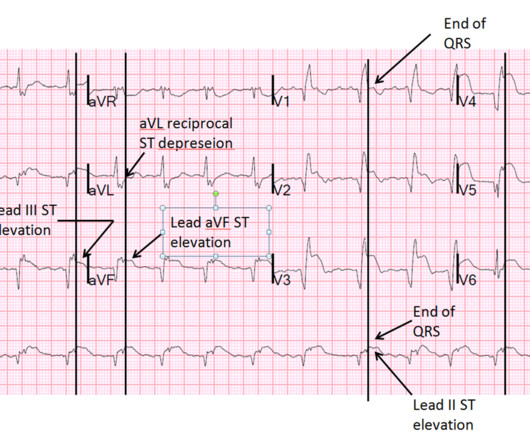
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. Another ECG was obtained during pacing: Mostly paced rhythm with PVCs (#3, #6, #9, #12). This is an obvious inferoposterior OMI.
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. Rather than using terms like “STEMI” and “Wellens”, it’s more helpful to describe the underlying pathology and ECG pattern pattern: Occlusion MI, and reperfusion T wave inversion 4. JAMA Intern Med 2019 9.
Then, 1 hour before arrival, it recurred, again lasting 5 minutes. There is STE that does not meet STEMI criteria in V1-V6. For clarity — I’ve put the 2 pieces of the 1st ECG together, and I’ve relabeled the tracings ( Figure-1 ). Figure-1: The first 2 ECGs in this case ( See text ). It lasted 5 minutes then resolved.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. per year incidence of SCD in this cohort [1]. Bicarb 20, Lactate 4.2,
Sent by anonymous, written by Pendell Meyers A man in his late 40s presented to the ED with concern for allergic reaction after accidentally eating a potential allergen, then developing an itchy full body rash and diarrhea. In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis.
There are two main etiologies of ischemic ST-depression: 1) subendocardial ischemia 2) reciprocal to ST-elevation in an opposite wall Here there are distinct R-waves with marked ST-depression throughout most of the precordium. But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
For clarity — I’ve put these 2 tracings together in Figure-1. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). The ECG finding that I KNOW is real in ECG #1 is the mirror - image appearance of ST-T waves in leads III and aVL.
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. normal variant, not pericarditis) A Young Man with Sharp Chest pain (normal variant, not pericarditis) 24 yo woman with chest pain: Is this STEMI? 15-9/6/2017 ). Pericarditis?
This is a 30-something healthy patient presented with COVID pneumonia who presented to the ED. Here they are: Learning Points: 1. In a series of 18 patients with COVID and ST elevation, 8 were diagnosed with STEMI, 6 of whom had an angiogram and it showed obstructive coronary disease. He was moderately hypoxic.
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. On arrival in the ED, he was hypotensive with a systolic blood pressure in the 70s. What is it?
The ED physician read this as "Normal sinus rhythm. It does not meet STEMI criteria. Obvious STEMI(+) OMI of inferior, posterior, and lateral walls, now with likely 2nd degree heart block type 1 (Wenckebach). In Figure-1 — The ST-T wave abnormality in lead V2 of ECG #1 is obvious. Easy for anyone.
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Learning Points: 1. What do you think? V1 has 0.5
Important Learning Point: "STEMI" is defined by millimeter criteria (1 mm in limb leads), which this does not meet. Therefore it is not a STEMI. But what we truly care about is coronary occlusion, for which STEMI is just a surrogate that is only about 75% sensitive for occlusion. Some are STEMI-equivalents.
Written by Pendell Meyers, edits by Smith and Grauer A man in his late 20s with history of asthma presented to the ED with a transient episode of chest pain and shortness of breath after finishing a 4-mile run. At the time of evaluation in the ED, his symptoms were resolved. Anterior STEMI? What is it? Activate the Cath Lab?
He presented to the ED because he developed sudden severe, sharp, pleuritic (but not positional), substernal and left mid to lower chest pain. I was relieved to see this MRI result: MRI IMPRESSION 1) Mildly decreased LV function with no focal wall motion abnormalities. Learning Points: 1. Pericarditis?
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 The patient arrived in the ED. The pain completely resolved after nitroglycerine Moments later, the this ECG was recorded in the ED when she had been pain free for moments only: Computer read: Normal ECG.
We obtained access and monitoring, but she showed no signs of improvement, and we judged that an intervention must be done in the ED without delay. The ED catheter was removed at that point and she did not require any further procedures. Ultimately, she spent several days in the hospital and no further fluid collected.
This is what the providers in the ED understood on patient arrival: Patient called 911 for syncope, then had witnessed PEA arrest after medics arrived. A 12-lead was recorded, showing "STEMI," but is unavailable. She was brought to the ED in a deep coma with GCS of 3, with vital signs, and an ECG was recorded: What do you think?
Whether your program is primarily 9-1-1, interfacility transport (IFT), or a combination of both, the likelihood of being responsible for the safe and expeditious transport of a STEMI patient is high for anyone in the out-of-hospital care setting. Here are my top 5 recommendations to add to your STEMI bundle of care.
A 43-year-old male with a history of mitral valve regurgitation s/p valvular replacement, hypertension, hyperlipidemia was evaluated in the ED for septic shock secondary to a pyelonephritis with a renal abscess. Chu CK, Delia E, Mograder A, Dwyer EM. 2017;45(1):12-20. 2015;7(9):E365-E369. J Saudi Hear Assoc. J Thorac Dis.
She arrived to the ED with a nonrebreather mask. The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Management?
Around the world, acute pain is the most common reason for patients to present to the emergency department (ED). 1 Regional anesthesia services are typically provided by anesthesiologists; however, there are various reasons why not all hospital models can support a dedicated service line run by anesthesiologists including physician shortage.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content