This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
[link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. EMS obtained the following vital signs: pulse 50, respiratory rate 16, blood pressure 96/49. cTnI drawn at the same was 0.011 ng/mL (ref.
When EMS found her, she was dyspneic and diaphoretic. The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. Figure-1: I've labeled the initial ECG in today's case. Her ECG is shown below: What do you think?
Guidelines recommend the use of validated risk models to estimate the risk of acute myocardial infarction , 30-days and 1-year mortality in patients with NSTE-ACS. TIMI Risk Scores for NSTE-ACS (NSTEMI, UA) and STE-ACS ( STEMI ) can be calculated below. TIMI, GRACE and PURSUIT are such risk models. Circulation.
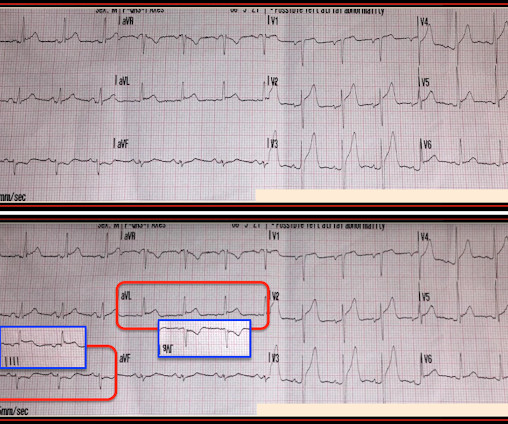
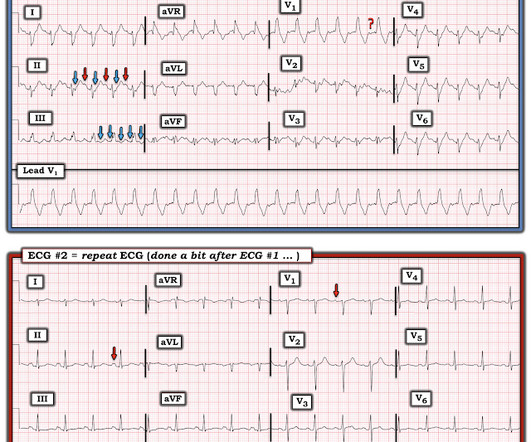
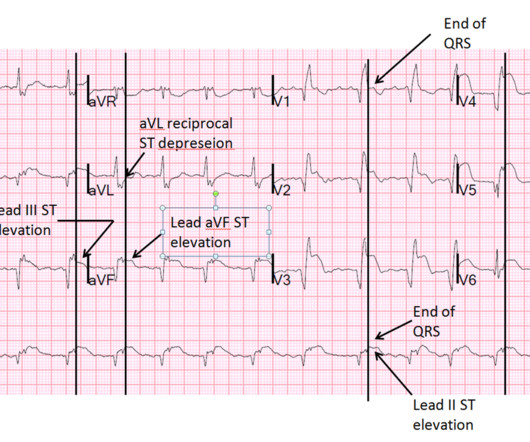
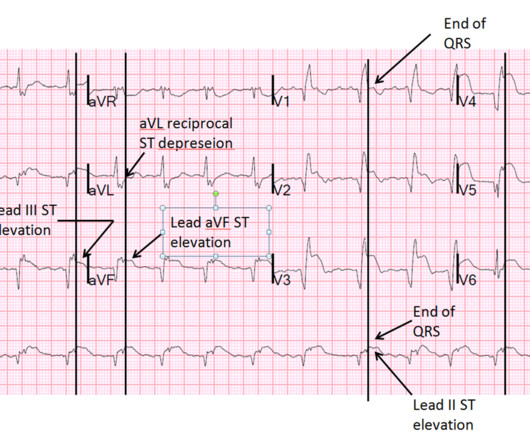
Her family called EMS and EMS recorded hypotension and this ECG: What do you think? There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. Another ECG was obtained during pacing: Mostly paced rhythm with PVCs (#3, #6, #9, #12). This is an obvious inferoposterior OMI.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 If you use something like the HEART score: 1. E EKG: a negative ECG (score = 0) 3. She was having a transient STEMI, briefly. Learning Points : 1. She called 911. A Age: = 0 4.
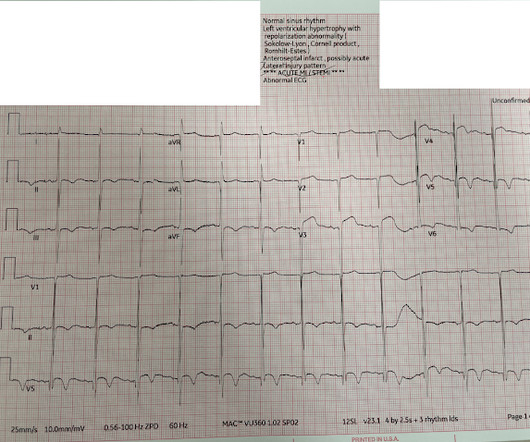
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case. After seeing ECG #2 — Can you explain: i ) Why no negative P wave was seen in lead V1 of ECG #1? —
He had walked into the ED (did not use EMS). Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. J Am Coll Cardiol 53(17):1503-9. Plum mer D, Dick C, Ruiz E, Clinton J, Brunette D.
He had walked into the ED (did not use EMS). Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Lessons : 1. Exact pain history was difficult to ascertain.
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." What do you think? VS on arrival: HR 95, BP 131/83, RR 14, SpO2 98%, Temp 36.7
She was ventilated by bag-valve-mask by EMS on arrival and was quickly intubated with etomidate and succinylcholine. The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. per year incidence of SCD in this cohort [1].
Submitted and written by Destiny Folk MD , peer reviewed by Meyers, Smith, Grauer, McLaren A man in his early 30s with no significant past medical history was brought to the ED by EMS after being found unresponsive by a friend. EMS arrived and found him awake and alert. They opined that the ECG could instead be "metabolic."
Even before we have clinical context, this ECG simply does not appear concerning for OMI, notwithstanding the machine's interpretation ** ** ACUTE MI / STEMI ** **. But in the world of STEMI, this is a challenging ECG to most. Pendell Meyers , Aaron E. I suspect most blog readers did not struggle with this one.
Authors: Rachel Bridwell, MD (EM Attending Physician; Tacoma, WA), Katey DG Osborne, MD (EM Attending Physician; Tacoma, WA) // Reviewed by: Alex Koyfman, MD (@EMHighAK, EM Attending Physician, UTSW / Parkland Memorial Hospital) and Brit Long, MD (@long_brit, EM Attending Physician, San Antonio, TX) Welcome to emDOCs revamp!
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chest pain and shortness of breath. The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. Also see these posts of Type II STEMI.
A 12-lead was recorded, showing "STEMI," but is unavailable. Moreover, if you know that catastrophic intracranial hemorrhage can result in an ECG that mimics STEMI, then you know that this patient probably has a severe intracranial hemorrhage. She was BVM ventilated and suctioned. Shortly thereafter, pulses were lost.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content