This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. Challenge QUESTION: The relative change in T-QRS-D is not the only thing that changes during period of time that passed between recording of the 2 ECGs shown in Figure-1.
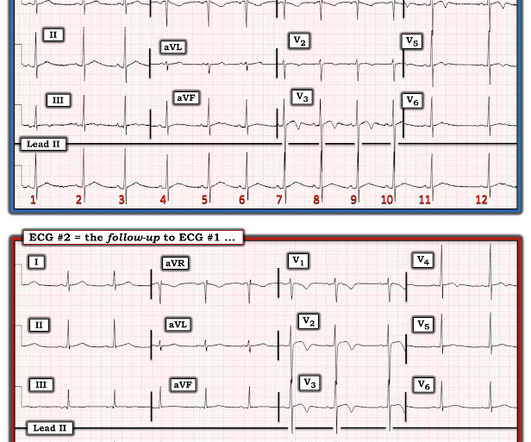
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT Coronary Angiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Day 12 ECG: FINAL DIAGNOSIS: "NSTEMI" Despite the fact that his day 4 ECG easily meets STEMI criteria, the patient is diagnosed as NSTEMI. No TIMI flow was listed in the report.
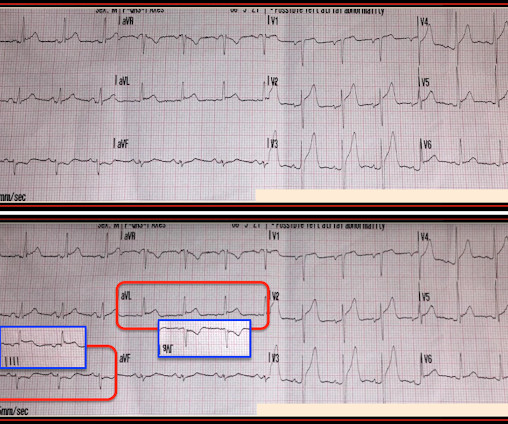
There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. The interventionalists insisted that the ECGs did not meet STEMI criteria and cancelled the activation, stating that they would consider urgent cath after further stabilization. This is an obvious inferoposterior OMI. mm STE with 9.5
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. Rather than using terms like “STEMI” and “Wellens”, it’s more helpful to describe the underlying pathology and ECG pattern pattern: Occlusion MI, and reperfusion T wave inversion 4. JAMA Intern Med 2019 9.
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Takotsubo is a sudden event, not one with crescendo angina. Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al.
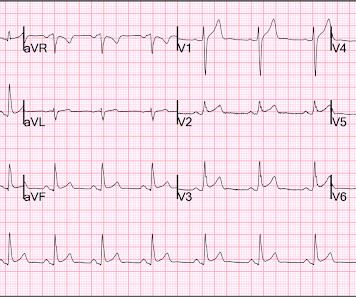
For clarity — I’ve put these 2 tracings together in Figure-1. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). The ECG finding that I KNOW is real in ECG #1 is the mirror - image appearance of ST-T waves in leads III and aVL.
Anterior STEMI? Regarding the History: It sounds from the History as if this patient has at least a significant component of EIA ( E xercise- I nduced A sthma ). It also sounds from events described that he was unaware of this possibility. What is it? Activate the Cath Lab?
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 If you use something like the HEART score: 1. E EKG: a negative ECG (score = 0) 3. Risk of 30-day adverse events is less than 1.7%. She was having a transient STEMI, briefly. Learning Points : 1.
S-wave is in V2 = 17 mm S-wave V4 = 9 mm Total = 26 (not greater than 28), so not LVH by the new rule! But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. For clarity — I’ve reproduced this ECG, to which I’ve made a few additions ( Figure-1 ). Peguero JG et al.
I found a well appearing young lady in the room with her parents who witnessed the event. She denied having any symptoms before or after the event, and she was asymptomatic on my initial exam. She was diagnosed with pericarditis and spent one day in the hospital without events. mm STE depression in aVL.
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
A prior ECG from 1 month ago was available: The presentation ECG was interpreted as STEMI and the patient was transferred emergently to the nearest PCI center. Patients that develop a Type 1 pattern without any precipitating or provoking factors have a risk of SCD of 0.5-0.8% per year incidence of SCD in this cohort [1].
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 11/2 hours. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. E CG # 1 = the initial Triage ECG ( TOP ) — As per Dr. Why is this important? Thelin et al.
Here they are: Learning Points: 1. 7 These 3 studies, as well as 1 smaller meta-analysis, 6 and another small study, 8 make it clear that troponin is associated with increased severity and mortality in COVID when adjusted for multiple other variables. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0
If you were thinking that this is not anterior OMI because there is no reciprocal ST depression , it is important to remember that half of anterior STEMI do NOT have any reciprocal ST depression. There are some unusual ECG findings in today's tracing ( that I labeled in Figure-1 ). Anterior OMI? Pericarditis?
The pattern of STE and STD reminded us of Brugada Type 1 morphology. Smith comment: 1) Brugada ECG may have ST shifts in limb leads as well as precordial leads. 2) The STE in V1 and V2 has an R'-wave and downsloping ST segments, very atypical for STEMI. per year incidence of SCD in this cohort [1]. Bicarb 20, Lactate 4.2,
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." That is a reasonable thought, but we have shown that if there is one lead of V1-V4 with a T/QRS ratio greater than 0.36, then it is STEMI, not LV aneurysm. Is this a transient STEMI? Learning Points: 1.
The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. Here are 9 cases that involve re-occlusion. If no, then she will tell you that the case is outside of the intended use group. In the November 27, 2024 post Drs.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Also see these posts of Type II STEMI. An EKG was immediately recorded.
Here is the written paramedic report available after all the events were over: Patient was seen by witnesses to become unresponsive. A 12-lead was recorded, showing "STEMI," but is unavailable. Today's patient unfortunately developed PEA ( P ulseless E lectrical A ctivity ) arrest shortly after arrival of the medic team.
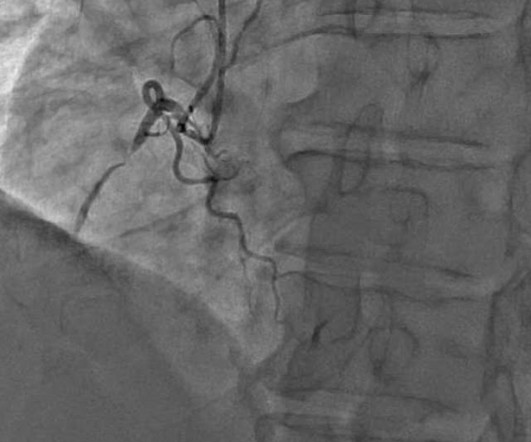
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. 1:51, diagnostic RCA angiography At this point, the patient very clearly has a diagnosis of OMI, especially since we visualized embolism within the PDA. & Falk, E. Papadopoulou, E., link] Falk, E., Bossone, E., Sharkey, S.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

























Let's personalize your content