This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
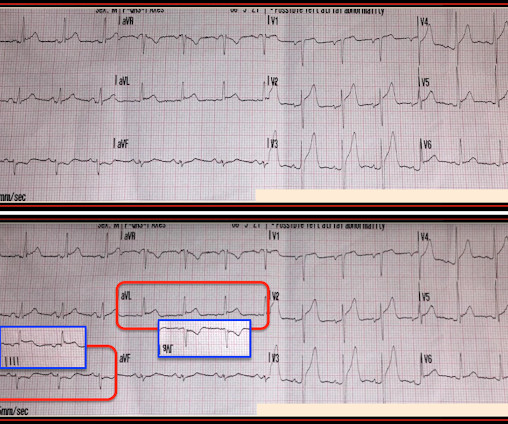
Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI." Case continued She was loaded with aspirin 325 mg, and repeat troponin drawn around the time of EKG 1 resulted at 267 ng/L. At midnight.
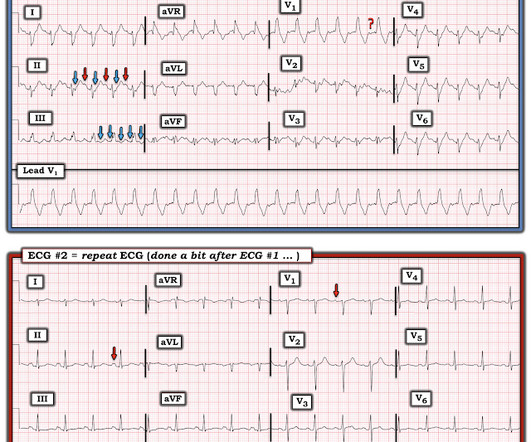
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). Figure-1: The initial ECG in today's case. After seeing ECG #2 — Can you explain: i ) Why no negative P wave was seen in lead V1 of ECG #1?
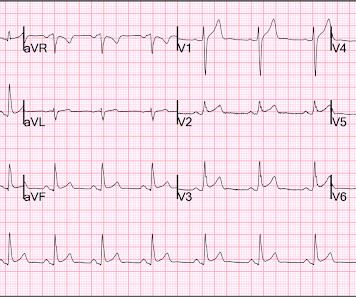
Pain improved to 1/10 after EMS administers 324 mg aspirin and the following EKG is obtained at triage. If this EKG were handed to you to screen from triage without any clinical information, what would you think? found normal ECGs in only 3 of 50 patients with massive PE, and 9 of 40 with submassive PE. What do you think?
Post cath ECG: Now there are hyperacute T-waves again, and recurrent ST depression in V2 This ECG would normally diagnostic of OMI until proven otherwise No further troponins were measured, but it looks like there is recurrent OMI Next day: A CT Coronary Angiogram was done (CTCA) CARDIAC MORPHOLOGY AND FUNCTION: 1. IMPRESSION: 1.
I texted this ECG with no information to Dr. Smith, who immediately said: "If CP, then anterior OMI until proven otherwise." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). No TIMI flow was listed in the report.
He had episodes of chest pain off and on all night, until about 1 hour prior to arrival when the pain became constant, crushing, 10/10 chest pain that radiated to both arms. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
Here it is: The computer reads STEMI What do you think? More from the medic: "LifePak 15 interpretation was STEMI. My response: "I think it is very worrisome for STEMI." It meets STEMI criteria even for a male under age 40, with STE 2.84 No history, meds, or risk factors. Pattern looked to be BER. mm in V2 and 4.08
Meyers comment: Ryan texted me this ECG with no information and my response was "Tough one. No further follow up information is available. For clarity — I’ve put these 2 tracings together in Figure-1. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3).
But these cases show the potential dangers of delayed recognition and treatment of inferior reperfusion Take away 1. Rather than using terms like “STEMI” and “Wellens”, it’s more helpful to describe the underlying pathology and ECG pattern pattern: Occlusion MI, and reperfusion T wave inversion 4. JAMA Intern Med 2019 9.
On review of systems the patient reported back pain for approximately 1 week which he was treating with NSAIDs with minimal relief. I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant." 15-9/6/2017 ). Pericarditis?
Here they are: Learning Points: 1. 7 These 3 studies, as well as 1 smaller meta-analysis, 6 and another small study, 8 make it clear that troponin is associated with increased severity and mortality in COVID when adjusted for multiple other variables. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0
mm of ST segment elevation, V2 and V3 have 1 mm of elevation, v4 has 2 mm of elevation and v5 around 1.5 Note 1: Levels were significantly lower in takotsubo that presented with T-wave inversion. Reference on Troponins: Xenogiannis I, Vemmou E, Nikolakopoulos I, et al. Learning Points: 1. What do you think? V1 has 0.5
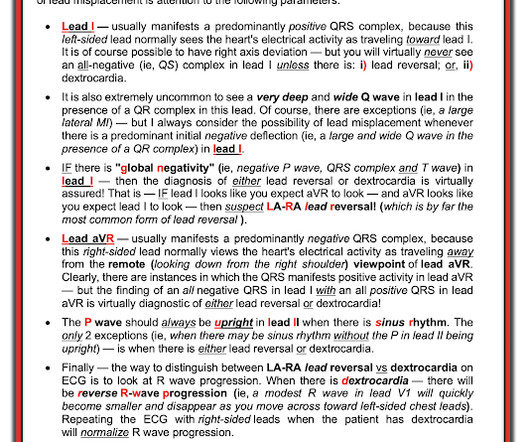
Despite the clinical context, Cardiology was consulted due to concerns for a "STEMI". Hyperkalemia mimics STEMI and OMI in many distributions, but probably the most common is the Brugada morphology in V1-V2 which mimics anterior OMI for those who cannot recognize the Brugada pattern. Limb lead reversal can be easily recognized.
If you were thinking that this is not anterior OMI because there is no reciprocal ST depression , it is important to remember that half of anterior STEMI do NOT have any reciprocal ST depression. If you were thinking that this is pericarditis, that would be possible in the absence of any clinical information. Pericarditis?
I was shown this ECG without any information: QTc = 431 ms What was my response? Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." Is this a transient STEMI? When Q-waves have developed, it cannot be assumed to be a transient STEMI. Learning Points: 1.
EMS recorded these prehospital ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 If you use something like the HEART score: 1. E EKG: a negative ECG (score = 0) 3. She was having a transient STEMI, briefly. Learning Points : 1. They give extremely valuable information.
The neurologic section was divided into (1) brain oxygenation, perfusion, edema, and intracranial pressure (ICP); (2) seizures and the ictal-interictal continuum (IIC); and (3) sedation and analgesia. Authors state early cath may be of benefit in those with no STEMI, but much of the more recent literature suggests this is more controversial.
They informed me that she had just been hospitalized 10 days ago for "some fluid around the heart" and was discharged after one day without incident. More specific information such as definitive RV diastolic collapse was not indicated or available at this time given the obvious clinical context. mm STE depression in aVL.
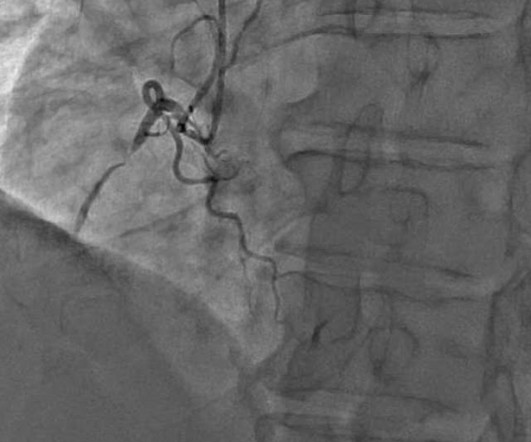
1:45, case start To orient you to this screen, the top is obviously ECG waveforms. 1:51, diagnostic RCA angiography At this point, the patient very clearly has a diagnosis of OMI, especially since we visualized embolism within the PDA. & Falk, E. Papadopoulou, E., link] Falk, E., Bossone, E., Sharkey, S.,
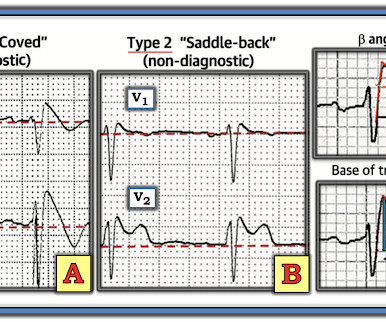
When I saw this (presented at a conference), I immediately thought it looked like Thype 1 Brugada phenocopy (in other words, Type 1 Brugada ECG pattern ). If the QRS is prolonged, then the differential includes: 1. Criteria for Type 1 Morphology: 1. A flat ST segment will have a Corrado index greater than 1.
1 Regional anesthesia services are typically provided by anesthesiologists; however, there are various reasons why not all hospital models can support a dedicated service line run by anesthesiologists including physician shortage. 9 The previous years volume of hip fractures was 569 patients. Morrison RS, Dickman E, Hwang U, et al.
The status of the patients chest pain at this time is unknown : EKG 1, 1300: There is sinus tachycardia and artifact of low and high frequency. I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content