This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
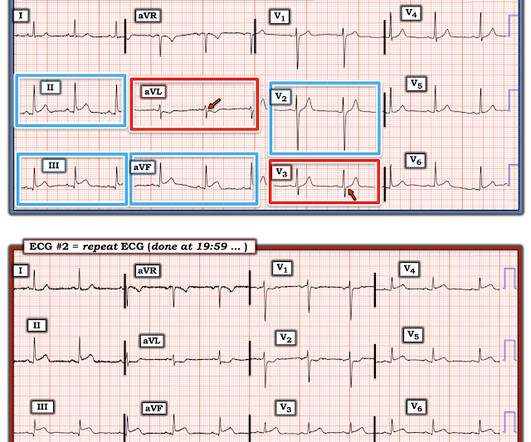
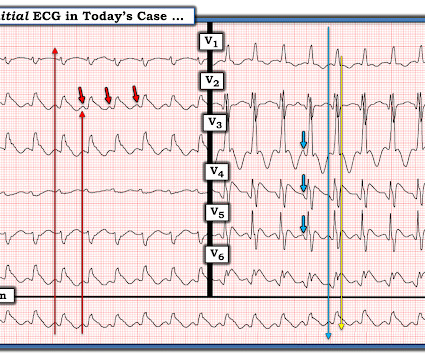
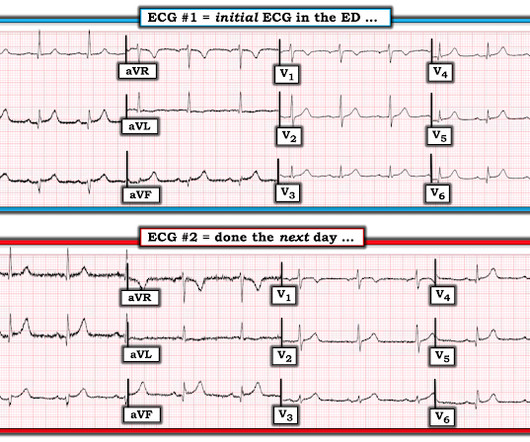
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
With a new protocol and Pulsara, Metropolitan Emergency Medical Services can now transport eligible pediatric behavioral health patients directly to behavioral health facilities—resulting in a 44% decrease of pediatric behavioral health patients transported to the ED. MEMS transports around 77,000 patients each year.
If you were working in a busy emergencydepartment, would you like to be interrupted to interpret these ECGs or can these patients safely wait to be seen because of the normal computer interpretation? have published a number of warnings about the previous reassuring studies.[4,5]
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. But according to Langlois-Carbonneau et al.,
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. This document covers high sensitivity troponin, risk disposition pathways, and STEMI equivalents.
Kaushal Khambhati is also a fourth-year resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. She arrives in the emergencydepartment (ED) with decreased level of consciousness and shock. She has a history of hypertension and non-insulin dependent diabetes mellitus.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Diagnosis of Type I vs. Type II Myocardial Infarction in EmergencyDepartment patients with Ischemic Symptoms (abstract 102).
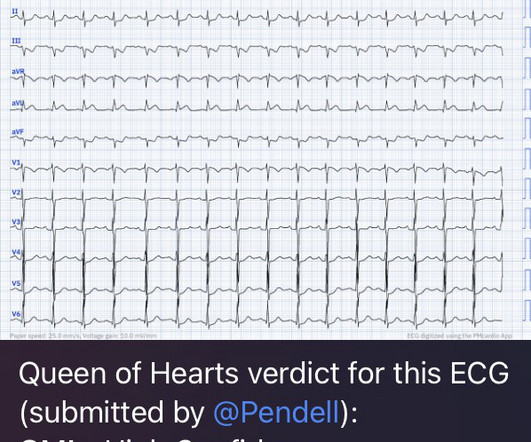
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby EmergencyDepartment where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Manual of Cardiovascular Medicine (5th ed.). Smith comment : V5 and V6 are excessively discordant!!!!
Written by Bobby Nicholson What do you think of this “STEMI”? A man in his 90s with a history of HTN, CKD, COPD, and OSA presented to the emergencydepartment after being found unresponsive at home. Vital signs were within normal limits on arrival to the EmergencyDepartment. Blood glucose was not low at 162 mg/dL.
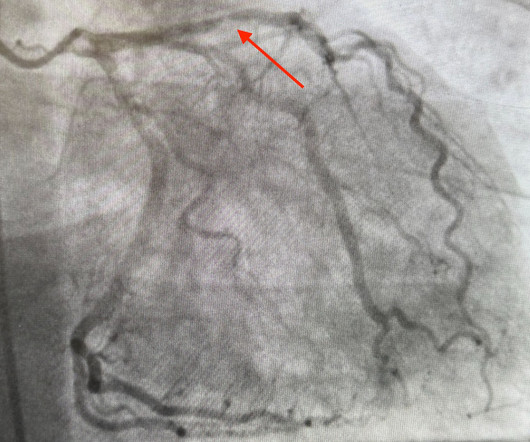
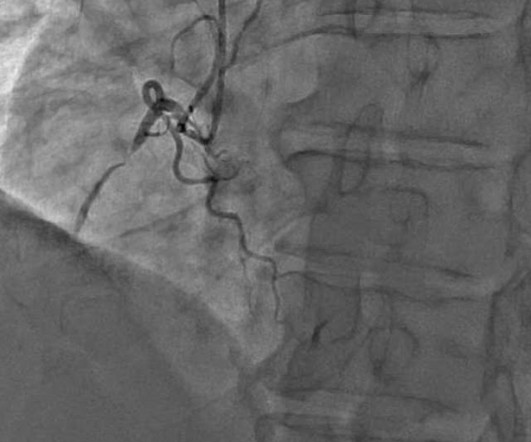
Now it is a full blown STEMI of 3 myocardial territories: inferior, posterior, and lateral But at least it does not call it "Normal." Learning Points: You cannot trust conventional algorithms even to find STEMI(+) OMI, even when they say "normal ECG." At this point — a STEMI was diagnosed, and cardiac cath with PCI was performed.
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. From Gue at al.
There is mixed overlap of ST-segment elevation (STE), ST-segment depression (STD), Hyperacute T waves (HATW), and deWinter pattern (which the ACC regards as a STEMI-equivalent but is better suited under the blanket of OMI). Western Journal of Emergency Medicine, 18 (4), 752-760. [2] link] [1] Zachary et al. 2] Costanzo, L. Physiology.
A 50 year old presented to the emergencydepartment of a remote rural community (where the nearest cath lab is a plane ride away) with one hour of mild chest pain radiating to the back and jaw, and an ECG labeled ‘normal’ by the computer interpretation. Figure-1: The first 2 tracings in today's case.
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 FIGURE 1: First ED EKG. FIGURE 2: Baseline ED from 2 months prior. FIGURE 3: Second ED EKG. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn. Click to enlarge.)
It was ongoing on arrival in the emergencydepartment. But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. The emergency physician was called to see the patient 90 minutes later after the troponin I returned at 1100 ng/L. What do you think? Take home 1.
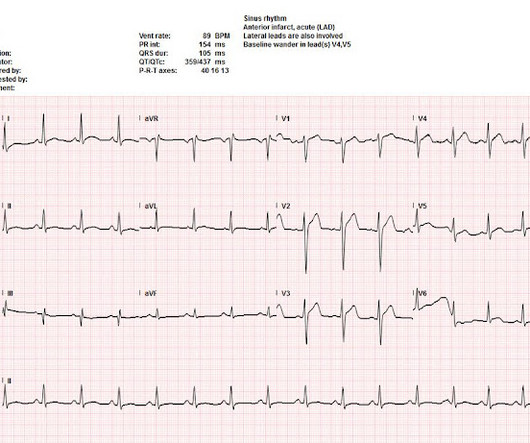
This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI.
52-year-old lady presents to the EmergencyDepartment with 2 hours of chest pain, palpitations & SOB. These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). In STEMI, they are generally upright and large in proportion to the QRS. So this argues against acute STEMI.
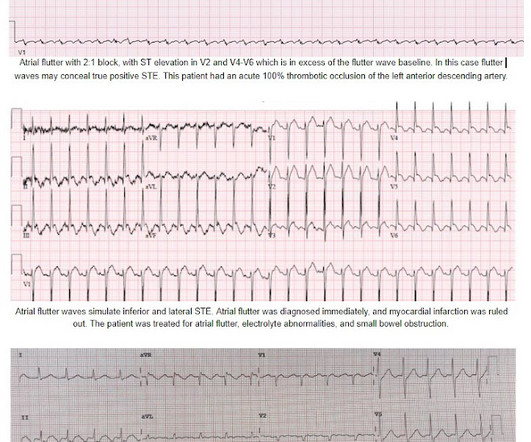
An ECG was recorded quickly on return to the ED: (sorry for poor quality, cannot get originals) What do you think? Is this inferor STEMI? Atrial Flutter with Inferior STEMI? The EM provider asked if the cardiologist thought it was a "STEMI." There is a narrow complex regular rhythm at a rate of approximately 120 bpm.
AslangerE A 65-year-old gentleman presented to the emergencydepartment after experiencing two recent ICD shocks in the preceding hours. This 65-year old male patient with severe underlying coronary disease presented to the ED after receiving several ICD shocks. That was also my initial concern.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Here is the first ED ECG, with no pain: Sinus rhythm.
Emergency physicians have earned the right to “re-brand” ourselves as indispensable, money-saving change agents in the health care enterprise. Of course, the bill for any episode of emergencydepartment (ED) care can be substantial, exceeding the billed charges for equivalent care provided in some primary care offices.
A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergencydepartment (ED). The patient initially presented to an outside ED and was subsequently transferred to our facility for continuity of care.
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high).
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Since then, I started looking for OMI EKG findings and not just STEMI. Case "Male, 43yo, come to ED with Epigastric Pain started 3 hours ago. Risk Factors: High Cholesterol.
One case sent by Dr. Sean Rees MD, written by Pendell Meyers, other case by Sam Ghali and Steve Smith Take a look at these two ECGs below from two patients in the ED, first without any clinical context. The remainder of his EmergencyDepartment stay was uneventful. Physician interpretation: "No STEMI."
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
This has been termed a “STEMI equivalent” and included in STEMI guidelines, suggesting this patient should receive dual anti-platelets, heparin and immediate cath lab activation–or thrombolysis in centres where cath lab is not available. aVR ST segment elevation: acute STEMI or not? aVR ST Segment Elevation: Acute STEMI or Not?
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Am J Emerg Med 2020 3. Backus BE, Six AJ, Kelder JC, et al.
His symptoms were reportedly resolved upon arrival to the ED. ED ECGs: 0814 0830 These show continued reperfusion with no evidence of reocclusion. I am going to code this as an acute STEMI as he had transient ST elevation which started to evolve in the emergencydepartment but I think this is most appropriately termed STEMI."
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? This one likely does meet STEMI criteria in II, III, and aVF. Criteria for a STEMI are definitely not met in ECG #1. What happened?
A middle-aged man presented with 7-8/10 non-radiating chest tightness to the left chest wall, associated with nausea but no diaphoresis, that began while walking approximately 40 minutes prior to arrival at the ED. The pain resolved as he arrived to the emergencydepartment. What do you think?
Study idea: We should look at all OMIs who had a chest CT and compare to all patients with Non-OMI pathology who had a contrast chest CT and have radiologists blindly interpret the perfusion of the myocardium The cardiology fellow came down to the ED and said: "What are you worried about? This ST depression?" 2022.08.750 Section 5.2.2,
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. Around 19 hours later, he experienced the same pain, which prompted his presentation to the ED.
She was unable to be defibrillated but was cannulated and placed on ECMO in our EmergencyDepartment (ECLS - extracorporeal life support). This is a troponin I level that is almost exclusively seen in STEMI. So this is either a case of MINOCA, or a case of Type II STEMI. Troponin I rose to 44.1
These kinds of cases were excluded from the study as obvious anterior STEMI. --QTc Case 1 Acute anterior STEMI from LAD occlusion, or Benign Early Repolarization (BER)? This is the initial ED ECG of a 46 year old male with chest pain: The QTc was 420 ST Elevation at 60 ms after the J-point in lead V3 = 2.5 100% LAD occlusion.
Emergent cardiac outcomes in patients with normal electrocardiograms in the emergencydepartment. Am J Emerg Med. These include about 60 occlusion MI (OMI) with clear ST segment elevation (none of which would be called “Normal” by the computer) and about 165 Non-STEMI. 2022 Jan;51:384-387. doi: 10.1016/j.ajem.2021.11.023.
The patient’s ECG on arrival at the emergencydepartment is shown below. Figure-1: The initial ED ECG ( = E CG # 1) — with comparison to the patient’s baseline ECG done 4 years earlier ( = E CG # 3). He was expected to arrive at the tertiary care center within 60 minutes of the call. No arrhythmias occurred en route.
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The screening physician ordered an EKG and noted his ashen appearance and moderate distress. Triage EKG: What do you think?
He presented to the ED because he developed sudden severe, sharp, pleuritic (but not positional), substernal and left mid to lower chest pain. Here is the parasternal short axis, performed by a real expert in emergencydepartment point of care cardiac ultrasound: There does not appear to be an anterior wall motion abnormality.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
The specific ST/T pattern was not fully appreciated by the attending EMS personnel, yet alarming enough to convince the patient to be seen in the EmergencyDepartment despite his intentions of seeking evaluation on his own accord through his respective family physician. it has been subsequently deemed a STEMI-equivalent.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content