This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These are high risk patients and they are high risk to you and your ED staff. The post Ep 115 EmergencyManagement of the Agitated Patient appeared first on Emergency Medicine Cases. It’s important to understand that agitation or agitated delirium is a cardinal presentation – not a diagnosis.
Aaron Orkin discuss the latest in naloxone in opioid overdose cardiac arrest and altered LOA, a 5-step approach to ED opioid withdrawal management and how we can improve mortality and morbidity in patients with opioid use disorder in the era of the opioid epidemic.
You contact ICU, anaesthetics, ENT, and oncology with a plan to attempt more definitive imaging in the prone position (which Ginny tells you is much comfier) What’s the evidence for our emergentmanagement? Arguably, more robust research is neither feasible nor ethical to conduct in such a rare and time-critical emergency.
Two classic EM Cases main episode podcasts, IV Iron for Anemia in EM with Jeannie Callum and Walter Himmel, and EmergencyManagement of Hyponatremia with Melanie Baimel and Ed Etchells are covered in the latest Rapid Reviews Videos by Taryn Lloyd and Nick Clarridge.
A 30 year old NIDDM is brought to your ED after being found with altered mental state following an argument with his partner. He is unwell, has compensated shock requiring emergentmanagement
6 24% more likely to return to the ED within 72 hours of their initial visit in an urban ED with >50,000 annual visits. 6 24% more likely to return to the ED within 72 hours of their initial visit in an urban ED with >50,000 annual visits. One cohort study in a public ED found that 84.5%
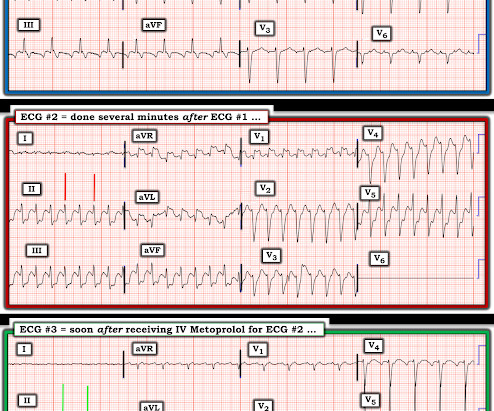
If I saw this patient in the ED, I would electrically cardiovert back to sinus rhythm. Additional Management Questions: The patient presented to the ED for palpitations — and was initially in AFlutter with 2:1 AV conduction. While these do not alter emergencymanagement of this patient's arrhythmia — They should be noted.
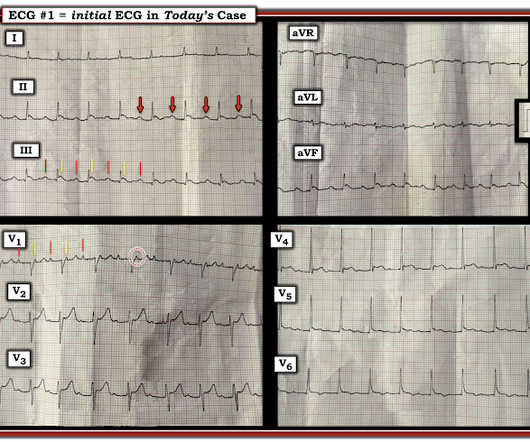
By Sofiya Diurba MD, reviewed by Meyers, Grauer A woman in her 50s with PMH known RBBB and prior syncopal events presents to the ED for five syncopal events over the last 24 hours. This is her first ECG in the ED: What do you see? Each event is associated with a prodrome of mild substernal CP, SOB, and “brain fog.”
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. Initial emergencymanagement is similar for both entities ). Triage ECG: What do you think?
The risk of a biphasic reaction is what keeps patients in the ED while being observed for a set period of time. Thus, if the patient has complete resolution of symptoms after appropriate treatment of anaphylaxis, there is no set time period for monitoring in the ED. This is called a biphasic reaction.
. == MY Comment , by K EN G RAUER, MD ( 7/7 /2024 ): == Among the most rewarding type of case for me during my days working in the ED — would be seeing a patient who presented with acute CP ( C hest P ain ) — who I would be able to “cure” simply by recognizing and treating their arrhythmia.
Data is being put front-and-center in the fire services industry with the implementation of the new National Emergency Response Information System (NERIS) by the U.S. Due to this, it’s important for the industry to develop strategies for better supporting psychiatric patients while avoiding unnecessary ED visits and secondary EMS transports.
If the hose is narrow, less water flows through (low current) References Electrocution and Electrical Injury – EmergencyManagement in Children; Children’s Health Queensland Hospital and Health Service Baird J. In: Walls RM, ed. Rosen’s Emergency Medicine: Concepts and Clinical Practice. Electrical Injuries.
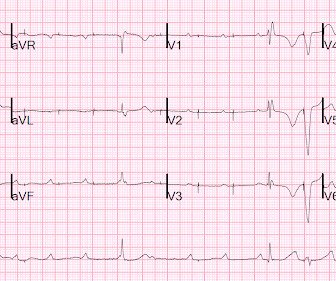
External pacing was attempted but not tolerated and, because the patient was only mildly hypoperfused, she was transported to the ED without further intervention. Here is the first ED ECG: What are you seeing? Try to figure it out before reading the explanation below. Treat hyperkalemia or drug toxicity 2. Treat ischemia (Cath lab) 3.
This single-centre academic urban institution in the United States (US) undertook a 10-year retrospective observational study of paediatric intubation and bougie use in their emergency department (ED). However, 273 were excluded, as 173 were intubated outside of ED, and 95 had missing datasets. years in the non-bougie group.
Among the presentations seen in the ED, few command the same respect as status epilepticus. Status epilepticus can be nuanced to manage. The post Ep 133 EmergencyManagement of Status Epilepticus appeared first on Emergency Medicine Cases.
The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED. This is less critical in EDmanagement of the unstable pelvic fracture, as the optimal site for identification of rectal or vaginal tears is the operating room.
Due to this, it’s important for the industry to develop strategies for better supporting psychiatric patients while avoiding unnecessary ED visits and secondary EMS transports. Mary’s Medical Center and Pam Beach Children’s Hospital and Garrett Hall , Sr.
The sensitivity of these scores range, but they cannot exclude FG diagnosis and may have lower sensitivity when used for prediction in ED patient populations. Fournier's gangrene and its emergencymanagement. 22 Computed tomography (CT) with IV contrast has a better sensitivity and specificity for NSTI, 88.5% Postgrad Med J.
ManagementEDmanagement should focus on appropriate resuscitation of the patient and early referral to the surgical team. Ensure appropriate bay allocation in ED. Pediatr Emerg Care, 1;38(6):e1332-e1335. How unstable is this patient? Do they need to be in the bay in front of your nursing station or in resus?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content