This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: February 28, 2024 Guest Skeptic: Dr. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Case: A 59-year-old man walks into your community emergency department (ED) complaining of chest pain.
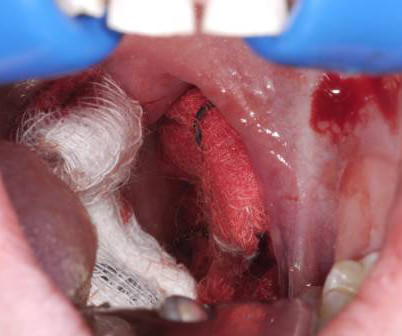
A young woman, 13 days post-tonsillectomy, comes into your rural emergency department (ED) coughing up blood. Managing post-tonsillectomy hemorrhage in the ED can be challenging, especially in rural or resource-limited settings. Hemoptysis ED approach and management. Its going to take time to get her to a tertiary center.
A narrow pulse pressure has been shown to predict the need for hemorrhage control in the ED setting but has not been assessed as a predictor in the prehospital setting. A narrow pulse pressure occurs due to compensatory increased systemic vascular resistance in the setting of decreased cardiac output.
We’ll keep it short, while you keep that EM brain sharp. A 70-year-old female with a past medical history of hypertension, coronary artery disease s/p 2x drug eluting stent placement one month ago, atrial fibrillation on apixaban presents to the ED with weakness and lightheadedness. F, RR 16, SpO2 97% on room air. J Emerg Med.
Children in the validation cohort were admitted to the intensive care unit or operatingroom less frequently than those in the derivation cohort. A proportion of the patients who were initially missed using the CDR were found to actually have risk factors documented in EMS reports or the medical record.
A 58-year-old male with a history of alcohol abuse presented to the emergency department (ED) as a category 2 trauma for a fall with a reported flail chest. EMS recognized a chest wall deformity with movement of the chest wall, and a splint was devised and taped around his chest for what was suspected to be a flail chest. J Surg Res.
This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so. The impact of push-dose phenylephrine use on subsequent preload expansion in the ED setting. 2015;10(3):e0119331. PMID: 25789927 Schwartz MB, et al. Am J Emerg Med. Am J Emerg Med.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergency department (ED) for an electrical injury and fall from a high voltage electrical pole. Per EMS, the patient was found at the bottom of a high voltage line with diffuse burns and amputation of his left forearm.
Over the past few years, there has been an increase in emergency department (ED) volumes and lengths of stay. The result of this ED capacity strain and less than ideal patient to staff ratios has led to delays in interventions, treatments and care adjustments. Paper: Owyang CG, et al. J Crit Care.
We’ll keep it short, while you keep that EM brain sharp. 1-3 Despite its commonality it retains a relatively high rate of complications overall and patients frequently present to the ED for evaluation. 10% of patient’s have an ED visit within 30 or 90 days following THA. 18 Fracture dislocations often managed operatively.
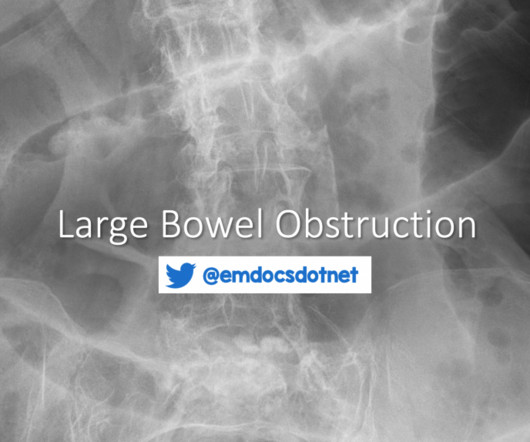
and is poorly tolerated by patients with obstruction, it should not be a routine part of the ED evaluation for LBO unless it is critical for another diagnosis on the differential. He describes the pain as a gradually worsening pressure-like discomfort distributed across his entire abdomen. He reports distension and the sensation of fullness.
C, respiratory rate 20 breaths per minute, and oxygen saturation 95% on room air. What is the EM physician’s role in the stabilization of unstable pelvic injuries? The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED.
Included patients from out-of-hospital, emergency department, intensive care unit, and operating-room intubations. Intubation performed in all settings (out-of-hospital, emergency department, ICU, and operatingroom). Randomized controlled trials or comparative non-randomized observational studies. in another study).
Rosens Emergency Medicine: Concepts and Clinical Practice, 7 ed. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. Rezaie, MD (Twitter/X: @srrezaie ) The post REBEL Core Cast 133.0 – TMJ Dislocation appeared first on REBEL EM - Emergency Medicine Blog. Louis, Mosby, Inc., 2010, (Ch) 70: p 895-909. GorchynskiJ et al.
An EM Residents Guide to Basic Airway Management Authors: Justin Rice, MD Sagar Desai, MD Eunice Monge, MD William Chiang, MD Preface: Airway management is one of the most critical skills in emergency medicine, yet it can be one of the most challenging to master. Introduction Airway management is a critical ED skill to master.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.















Let's personalize your content