This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Let’s consider Inborn Errors of Metabolism Presenting in the ED : Inborn Errors of Metabolism: Basics Common Presentations, Uncommon Kiddos For the child with lethargy, vomiting, acidosis, hypoglycemia , organomegaly, or cardiopulmonary arrest remember to consider Inborn Errors of Metabolism (IEM) on your DDx. Samantha A.
How and when to reverse anticoagulation in the bleeding EM patient. Comparison between Prothrombin Complex Concentrate (PCC) and Fresh Frozen Plasma (FFP) for the Urgent Reversal of Warfarin in Patients with Mechanical Heart Valves in a Tertiary Care Cardiac Center. Iran J Pharm Res. 2015;14(3):877-885.
It is commonly missed during the first few ED visits. First line therapies for anti-NMBDA receptor encephalitis consists of… High dose steroids , IVIG, and PLEX – Therapeutic plasma exchange Only 50% of patient’s respond, and will require second line therapies such as Rituximab. Moral of the Morsel It’s NOT always psych!
Case: A 62-year-old man is brought in by EMS from home with lethargy and hypotension. sodium chloride), and balanced crystalloid solutions, meaning those with a chloride composition closer to plasma such as lactated ringer’s or Plasma Lyte 148. Early work suggested potential harm from 0.9% We reviewed that last time on SGEM#347.
Now, let’s discuss another complication of “The Great Mimicker” which may throw us for a loop in the ED – Pseudoparalysis of Parrot : Pseudoparalysis of Parrot – Basics First described by Jules Marie Parrot in 1871. The post Pseudoparalysis of Parrot appeared first on Pediatric EM Morsels. Index of Suspicion. Pediatr Rev.
We’ll keep it short, while you keep that EM brain sharp. A 37-year-old G2P2 female with no other past medical history presents to the ED with a 2-day history of intermittent fever and foul-smelling vaginal discharge. Plasma cell endometritis is associated with Chlamydia trachomatis infection. What is the diagnosis?
He is also now a fully fledged “sonologist” Casey currently splits his time between Broome, a small rural hospital in the remote Kimberley region of Western Australia, and a large tertiary ED in sunny Perth. They have two large bore intravenous (IV) access and are planning to bring them to your ED as soon as possible.
Case: A 71-year-old man is brought to your emergency department (ED) by emergency medical serviced (EMS) having fallen two steps at home. EMS have already splinted an obvious mid-shaft femoral fracture, but he continues to be tachycardic and hypotensive. years ( 2 ).
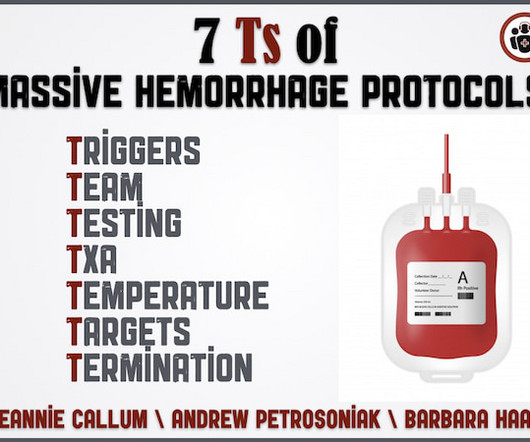
Why is serum calcium important to draw in the ED for the patient who is exsanguinating? If someone is on anti-platelets or anticoagulants what is the best strategy to ensure the docs in the ED know what to give and how much? What should be the lab resuscitation targets? How do we mitigate the risk of hypothermia? When and how much TXA?
It's important to keep in mind that you are not functioning as an EMT when you're an ED Tech/Assistant. So when it comes time to renewing your certification or license, you'll have to directly correspond with the IDPH rather than an EMS Coordinator within a system. The biggest event they provide EMS for recently is Lollapalooza.
Bradykinin Mediated Plasma globulins called kininogens release bradykinin and cause vascular permeability. Image: ( Morgan 2010 ) Features Absence of urticaria and pruritus Insidious onset (24-36 hours) ACE Inhibitors Inhibition of ACE hinders the degradation of bradykinin and can lead to idiosyncratic angioedema.
Case: A 66-year-old woman is brought in by EMS from home with lethargy and hypotension. Some bench work, observational studies, and now two large, unblinded, cluster-randomized single-center trials ( SMART and SALT-ED ) suggested a benefit to using balanced crystalloids (i.e. Lactated Ringer’s or Plasmalyte 148) over 0.9%
Authors: Alex Rogers, MD (EM Resident Physician, Christus Spohn/Texas A&M University School of Medicine, Corpus Christi, TX); J.D. These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. lidocaine) or an ester (e.g.,
Congenital Syphilis may still occur in patients presenting to your ED! The post Congenital Syphilis appeared first on Pediatric EM Morsels. Can identify T. pallidum before antibodies against it can be detected. > 4 weeks of age : Aqueous crystalline penicillin G 50,000 Units/kg IV every 6 hours Treat for 10-14 days. Emerg Radiol.
3 Measured in analytical testing : Laboratories measure plasma concentration using osmometers which measures values as a function of kilograms of solvent. Choice of the best equation for plasma osmolality calculation: Comparison of fourteen formulae. Validation of equations used to predict plasma osmolality in a healthy adult cohort.
JAMA 2015 [7] The PROPPR Trial 680 severely injured adult trauma patients Patients randomized to Plasma, Platelets, and PRBCs in a 1:1:1 ratio vs 1:1:2 ratio No difference in overall mortality at 24 hrs BUT 1:1:1 achieved hemostasis faster and fewer experienced death due to exsanguination at 24hrs Crombie N et al. Ann Emerg Med.
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. The trauma call goes out. You will be running the show today, and you want to use your preparation time well. to −0.5%]; P = 0.03.). to −0.5%]; P = 0.03.).
Authors: Amelia Campbell, MD (EM Resident Physician, Carl R. Darnall Army Medical Center) and Alec Pawlukiewicz, MD (EM Attending Physician, Carl R. Case: A 45-year-old woman presents to the emergency department (ED) with itching to bilateral palms. Her triage vitals are within normal limits. How does cholestasis present?
DEG is rapidly absorbed when ingested and can reach peak plasma and brain tissue concentrations within four hours of ingestion. “Diethylene Glycol” in Goldfrank’s Toxicologic Emergencies , 11e Eds. “Fomepizole” in Goldfrank’s Toxicologic Emergencies , 11e Eds. Schier, Capt. Nelson, et al.
2 TTP often presents abruptly, and most patients that develop it first visit the emergency department (ED) as their symptoms worsen. 1 Pregnant patients are particularly vulnerable to misdiagnosis of TTP in the ED. Most of these deaths can be attributed to a delay in diagnosis. Thus, early management is essential for patient outcomes.
Schnapp, MD, MEd (Associate Program Director, University of Wisconsin) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF), Marina Boushra (EM-CCM, Cleveland Clinic Foundation); Brit Long, MD (@long_brit) Case A 36-year-old pregnant woman at 21 weeks gestation presents to the ED with chest pain.
The midwives report that EMS is not needed for the baby. But, from a basic care perspective, I am not sure there is anything that the average EMS crew would do differently, despite this case being anything but basic. The midwives go on to explain that following the baby’s birth, the patient began to hemorrhage.
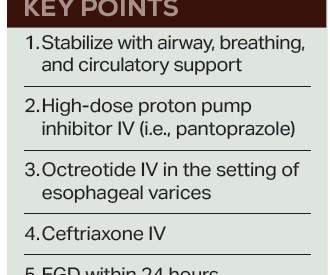
Fresh frozen plasma, or FFP, should only be given to cirrhotic patients as part of the massive transfusion protocol in cases of profound hypotension, as “patients with cirrhosis rarely have true enzymatic hypocoagulability, and FFP may worsen bleeding due to over-resuscitation and dilution of coagulation factors.” 6 Balloon tamponade (i.e.,
What is the EM physician’s role in the stabilization of unstable pelvic injuries? The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED. Her initial vital signs are blood pressure 76/54 mmHg, heart rate 128 bpm, temperature 37.0˚
Today, she would not get out of bed, prompting the facility to call EMS. On arrival to the ED, her blood pressure is 84/36 mmHg with a heart rate of 110 beats per minute. 3,4 Prompt recognition and management of sepsis and septic shock are paramount for the ED clinician. She had a fever of 38.7 °C F) in the ambulance.
EMS report was that the patient had unknown down time with unwitnessed arrest, found initially in VFib arrest, defibrillated x1 followed by PEA arrest alternating with asystolic arrest during transport. Terbutaline and Albuterol for Lowering of Plasma Postassium Initial labs returned and confirmed critical hyperkalemia and new renal failure.
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. These are send-out labs with turn-around times that make them unlikely to affect the ED course or guide treatment. CorePendium.
These are send-out labs with turn-around times that make them unlikely to affect the ED course. This prevents ongoing exposure to the patient and ED staff. In: Mattu A and Swadron S, ed. 3 However, may be helpful in diagnosing the chronic toxicity forms. Iran Red Crescent Med J 16: e5072, 2014. Pesticides and Cholinergics.
This would be a send-out test and would be unlikely to help us acutely in the ED. However, in extreme cases with highly toxic levels, one could consider plasma exchange if no other suitable alternative exists. 6 Urine heavy metals screens are not recommended for asymptomatic patients.
Collins, MD (EM Resident Physician, San Antonio, Texas); Michael J. Treatment requiresaggressive anticoagulation, glucocorticoids, plasma exchange, and intravenous immunoglobulin (IVIG)(27). This leads to adiffuse hypercoagulable state and widespread vascular dysfunction. anticoagulation and blood pressure control). Ann Rheum Dis.
A 33-year-old male with a history of drug use presented to the emergency department (ED) for extreme agitation after receiving two doses of 2 mg naloxone by EMS for respiratory depression. If available, an in-house ED pharmacist is an incredible resource for guidance when there are questions regarding pharmacologic management.
On arrival to the ED the patient’s initial vital signs are temperature 38.5C, BP 102/48, HR 106, RR 20. Antidote : Deferoxamine is a chelating agent derived from Streptomyces pilosus ; binds free iron from plasma and iron inside of cells. Coagulopathy: Parenteral vitamin K and/or fresh frozen plasma (FFP) as clinically indicated.
Authors: Gaston Omba, MD (EM Resident Physician, Makerere University); Jessica Pelletier, DO (EM Education Fellow, Washington University in St. How is this condition diagnosed and treated in the ED? Kirk M, ed. Laboratory testing was not immediately available. Trop Med Infect Dis. 2023;8(3):169. 2013;8(1):e54395.
An EM Residents Guide to Basic Airway Management Authors: Justin Rice, MD Sagar Desai, MD Eunice Monge, MD William Chiang, MD Preface: Airway management is one of the most critical skills in emergency medicine, yet it can be one of the most challenging to master. Introduction Airway management is a critical ED skill to master.
Well keep it short, while you keep that EM brain sharp. He was transported from the scene by EMS. Although the concentration of chloride in the CSF is slightly higher than in plasma, measuring chloride (B) is not an accurate way to detect the presence of CSF. However, he has a headache that has become more painful.
We’ll keep it short, while you keep that EM brain sharp. A 51-year-old male with a history of AIDS presents to the ED accompanied by his partner with complaints of cognitive decline and confusion over one month. ED Evaluation Neurosyphilis is known as a “great imitator” due to the extensive variability of nonspecific symptoms [11].
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 She is sent to the medical ward after three days in the ED with the diagnoses of resolving septic shock, severe malaria, and AKI.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content