This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Upon EMS arrival, they find the patient is sweaty with normal vital signs. AEM November 2023.
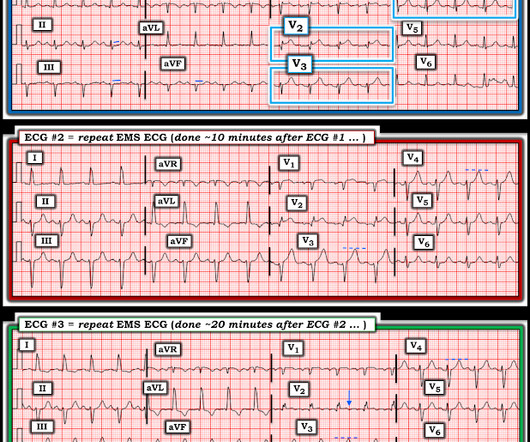
Written by Pendell Meyers A woman in her 70s had acute chest pain and called EMS. On arrival, EMS recorded relatively normal vital signs and this EMS ECG: What do you think? The EMS crew recorded another ECG about 10 minutes later (unknown if pain changed): New LAFB. So the cath lab was not activated. Ongoing OMI.
With a new protocol and Pulsara, Metropolitan Emergency Medical Services can now transport eligible pediatric behavioral health patients directly to behavioral health facilities—resulting in a 44% decrease of pediatric behavioral health patients transported to the ED. MEMS transports around 77,000 patients each year.
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Post Created By: William Caputo MD Post Peer Reviewed By: Anand Swaminathan MD, MPH (Twitter @EMSwami ) The post REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion appeared first on REBEL EM - Emergency Medicine Blog.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" He diagnosed anterior "STEMI" and activated the cath lab. What do you think?
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. It’s unclear if the paramedic ECGs were seen or missed in the ED. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. At this point the emergency physician asked for a stat cardiology consult.
From April 2-5, the top fire services and EMS industry thought leaders and data analysts gathered at Wave 2024 to share what trends they’re forecasting for both fields and how they’re enacting change within their own organizations through the power of data-driven insights. Data impacts every aspect of duties, from shifts start to end.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chest pain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
He called EMS who brought him to the ED. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. ED Diagnoses: 1.
Episode 86: Tricky Cases Part 2 Case 3: 56-year-old female with history of seizures, actively seizing, EMS called. Patient seized for approximately 20 minutes prior to EMS arrival. On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Every airway requires a plan and backups.
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. No troponins were measured!
Fire/EMS crews found him clammy and uncomfortable. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. But until its magic is available at bedside the clinician must train his/her eyes to spot the subtle features of OMI, and equally allow the bias of STEMI to fossilize.
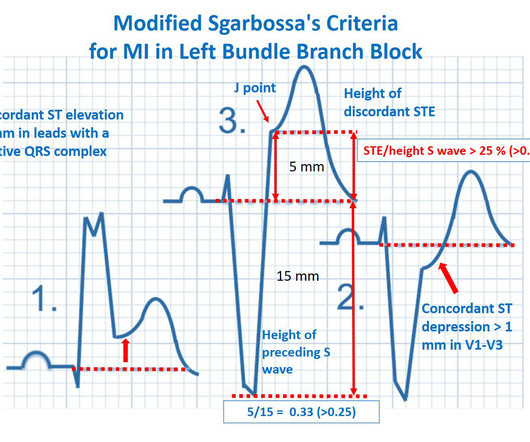
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI.
In EM Cases' first ECG Cases blog we review 7 examples of ECGs of patients presenting to the ED with chest pain, who's ECG were read as normal by the computer. And guess what.they all show acute ischemia!
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. Here is the final ECG just prior to ED transfer.
Jason was very skeptical of STEMI. This also argues against STEMI. Turns out that the patient regularly called EMS for complaints of chest pain that frequently led to cath lab activation.) He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree. V4 especially looks like early repolarization.
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. The patient was transported to the ED. Here is his ED ECG: There is sinus tachycardia. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
A 60-something woman called EMS for chest pain. Waiting to cath a transient STEMI can be hazardous. In the only ED study of its kind, sensitivity increased from 46% to 62%. This case comes from Jason Winter, of The Facebook Clinical Electrocardiology ECG Page. Here is her first prehospital ECG: What do you think?
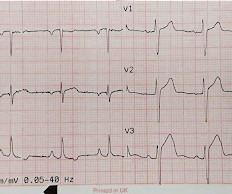
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Do either, both, or neither have occlusion MI? Vitals were normal.
Written by Bobby Nicholson What do you think of this “STEMI”? With EMS, patient had a GCS of 3 and was saturating 60% on room air. He improved to 100% with the addition of non-rebreather, however remained altered and was intubated by EMS with ketamine and succinylcholine. or basilar ischemia. There is high QRS voltage.
He has a history of STEMI and heart failure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. On arrival in the ED, the patient denied any symptoms at all. Figure-1: The initial ECG in today's case — obtained by the EMS team. ( A 50-something had syncope while driving.
EMS arrived and recorded this ECG: What do you think? Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case.
EMS arrived and found him in Ventricular Fibrillation (VF). The patient was brought to the ED and had this ECG recorded: What do you think? Cardiac arrest #3: ST depression, Is it STEMI? They started CPR. He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. sodium bicarbonate.
EMS showed us their ECG on arrival at her house: What do you think? There is sinus rhythm with minimal STE in V1-V3, not meeting STEMI criteria. The cardiologist arrived quickly and was skeptical about these findings on EMS ECG. The delay between OMI and STEMI sometimes causes unacceptable loss of myocardium or worse.
He presented to EMS with extreme pallor, Levine sign, diaphoresis, bilateral arm pain, and an apprehensive sense of doom. Chou's Electrocardiography in Clinical Practice, 6th ed. David Didlake, NRP, APRN, ACNP-BC This case is provided by C. Madden, Paramedic. Many thanks for sharing! Hyperkalemia revisited. 4] Surawicz, B. McCance, K.
When EMS found her, she was dyspneic and diaphoretic. The conventional machine algorithm interpreted this ECG as STEMI. See this post of RV MI with both McConnell sign and "D" sign: Inferior and Posterior STEMI. She was out walking her dog when she developed sudden dizziness and light-headedness. As per Dr.
He awoke from sleep with crushing central chest pain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. This male in his 40's had been having intermittent chest pain for one week. Type B waves are deeper and symmetric. A stent was placed.
Written by Pendell Meyers A middle aged man called EMS for acute chest pain. EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I said "Not OMI.
The case below was contributed by Pendell Meyers, an EM G1 at Mt. Validation of the Modified Sgarbossa Rule for Diagnosis of STEMI in the Presence of Left Bundle Branch Block. His ED ECG showed his baseline LBBB, with no evidence of MI. Sinai (the case did not come from Mt. Sinai though!) Limkakeng AT. Theiling BJ.
This was a middle aged female with a h/o CAD who presented to the ED by EMS sudden onset of central chest pressure 45 min prior to ED arrival with associated diaphoresis and SOB. There is LVH and there are ST-T abnormalities (large inferior T-waves and ST elevation, with reciprocal findings in aVL).
One of these areas is assessing patients with ED-diagnosed strokes. Working towards better detection Another area ESO has identified as an opportunity to improve is how EMS services detect a possible STEMI or NSTEMI with a 12-lead EKG. Improving the numbers So how can EMS services work together to improve these numbers?
Her family called EMS and EMS recorded hypotension and this ECG: What do you think? There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. This is an obvious inferoposterior OMI.
EMS found him with an irregular heart rate at 200-250 beats per minute. Upon arrival to the ED, he had the following 12-lead ECG: There is striking ST segment elevation in V1 and V2, with ST depression in V3-V6 as well as I, II, and aVF. He subsequently had a syncopal event and was down for 1-2 minutes. His wife called 911.
Figure 1-1 My colleague, a faithful student of ECG interpretation, handed me the tracing and said that it warranted STEMI activation because of apparent terminal QRS distortion (TQRSD) in V2. ASA 324mg was administered while a STEMI activation was simultaneously transmitted to the nearest PCI center. Attached is the first ECG.
EMS arrived and administered aspirin and nitroglycerin. Here are his three EMS ECGs: EMS1 at 0735 This was sent to Dr. Smith with no other information. His symptoms were reportedly resolved upon arrival to the ED. ED ECGs: 0814 0830 These show continued reperfusion with no evidence of reocclusion. Do not miss them!
Step 1 to missing posterior MI is relying on the STEMI criteria. A prospective validation of STEMI criteria based on the first ED ECG found it was only 21% sensitive for Occlusion MI, and disproportionately missed inferoposterior OMI.[1] But it is still STEMI negative. A 15 lead ECG was done (below).
This case was contributed by Brooks Walsh, an ECG enthusiast who has contributed frequently , and edited by Smith Case An elderly male called EMS after he developed “indigestion.” He was almost asymptomatic when he arrived in the ED. The paramedic interpreted this as a STEMI. Can you employ the Subtle Anterior STEMI calculator
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content