This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Their hospital has struggled with a growing number of adverse events that often occur without warning. With emergency department (ED) volumes rising, administrators are eager to explore AI-driven solutions to improve patient safety and reduce staff burnout. Reference: Verma et al.
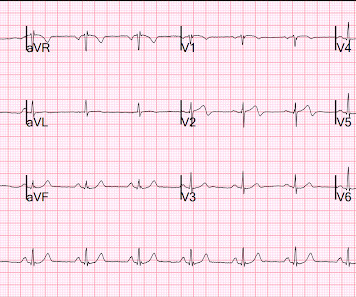
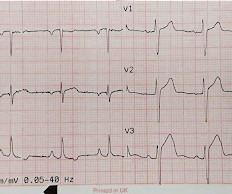
At the time of ED arrival he was alert, oriented, and verbalizing only a headache with a normalized BP. He denied any specific prodrome of gross palpitations, however did endorse feeling quite dizzy just before the event. The ED activated trauma services, and a 12 Lead ECG was captured. The fall was not a mechanical etiology.
The emergency department (ED) evaluation reveals an unremarkable chemistry panel with normal renal function and a white blood cell count of 10,000. Background: We have discussed agitation in the ED on the SGEM several times. They are afebrile and tolerate oral intake. These conflicts can ultimately lead to moral injury [1,2,3].
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He arrived to the ED by ambulance at 1529, only a half hour after the start of his chest pain around 1500 while eating. Patient 2 , EKG 1: What do you think? The patient had none of these conditions.
Yoo, MD (Assistant Professor/Core Faculty, San Antonio, TX) // Reviewed by Brit Long, MD (@long_brit) Case An 18-year-old man with a history of asthma and medication noncompliance presents to the emergency department (ED) with acute onset shortness of breath. He states that he recently moved to Texas from Colorado. Which one do you select?
Clinical Question: Does simultaneously performing the modified valsalva maneuver and administering intravenous adenosine, compared to either treatment alone, have greater success in achieving normal sinus rhythm in patients presenting to the ED with PSVT? This absence of detail leaves the study open to bias.
Today’s video evaluates inhaled corticosteroids (ICS) for asthma in the ED setting. EBM Updates: Inhaled Corticosteroids for Asthma in the ED Background : Asthma is a common ED issue, with patient presentations ranging from needing a medication refill to severe exacerbation in respiratory failure.
He called EMS who brought him to the ED. ED Diagnoses: 1. The basic principles of emergency ECG interpretation in patients who present to an ED with new symptoms include the following: Respect the History. This history immediately places this patient in a high -prevalence population for having an acute event.
Pathophysiology Primary injury happens at the time of the traumatic event or shortly after in the high cervical to mid-thoracic spine. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Tenenbein M, Macias CG, Sharieff GQ, et al, eds. Refers to the Spinal Cord Function and Reflexes, not specifically hemodynamic issues.
In many emergency departments (ED), US machines are readily available and can be used to rapidly assess and monitor patients with acute dyspnea at the bedside. US, compared with CXR and CT, offers the absence of ionizing radiation and high reproducibility. Emerg Med J. 2023;40(10):700-707.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
Annie: I developed an interest in EM while working as a scribe in the ED during college. In addition to what Charlotte and Nick said, I can envision myself staying calm in the stressful situations that come up in the ED. Nick: Triaging your time and priorities as an ED doc on shift is so challenging.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
This is Bob’s eleventh visit […] The post SGEM#291: Who’s Gonna Drive you to…the ED – with Lights & Sirens? July 2019 Guest Skeptic: Dr. Robert Edmonds is an emergency physician in the US Air Force in Virginia. first appeared on The Skeptics Guide to Emergency Medicine. Date: April 24th, 2020 Reference: Watanabe et al.
It's important to keep in mind that you are not functioning as an EMT when you're an ED Tech/Assistant. Standby EMS for events The company that comes to mind in Chicago is Event Medical Solutions. The biggest event they provide EMS for recently is Lollapalooza. It opens many doors in various industries.
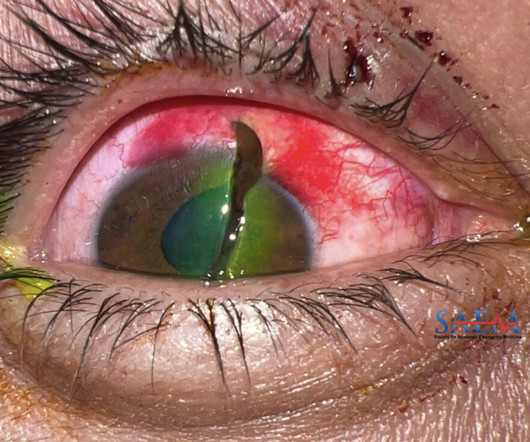
A 32-year-old male with no significant past medical history presented to the emergency department (ED) from an outside hospital for further management of right eye pain and vision loss sustained after he was struck by a metal wire while at work. He had no other complaints and denied any other trauma or loss of consciousness during the event.
In this issue, we collaborated with the CJEM team to present “Hypotension and respiratory events related to electrical cardioversion for atrial fibrillation or atrial flutter in the emergency department” in a visual abstract format1.
Provide a network system of centers to facilitate international cooperation in the event of national or manmade disasters. Each conference includes plenary sessions and speakers from around the world, pre-conference workshops, an exhibition hall, social events, and the opportunity to become involved in special interest groups (SIGs).
A 68-year-old man presents to the emergency department (ED) with altered mental status and fever. The study found a mean increase in time to intubation of 13 seconds in the ED setting. Vital signs on arrival are: Temperature: 38.8 He has an absent gag reflex. There was no analysis of operator experience or expertise.
However, ketamine may be associated with adverse clinical events including a higher intubation rate. The primary endpoint was incidence of endotracheal intubation occurring during transportation and within one hour after arrival to the emergency department (ED). versus 2.9%, respectively; p = 0.383).
Case: A 41-year-old man without a significant past medical history presents to the emergency department (ED) with a chief complaint of lower back pain that started 48 hours prior to the ED visits after attempting to move a couch in his house. Background: Pain is one of the most frequent reasons to attend an ED.
Case: A 15-year-old male presents to the pediatric emergency department (ED) with right ankle pain sustained while twisting his ankle during dance practice. Background: Pediatric emergency department (ED) visits and related procedures can invoke pain and anxiety among children. The right ankle is swollen and tender.
I interpreted this tracing knowing only that the patient was a woman in her 60s, with a prior history of proximal LAD OMI — who now presented to the ED with a history of new chest discomfort and shortness of breath. For clarity in Figure-1 — I’ve labeled today’s initial tracing. Figure-1: I've labeled the initial ECG in today's case.
Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Major adverse cardiac event rates in moderate-risk patients: Does prior coronary disease matter? Case: You are working a shift in your local community emergency department (ED) when a 47-year-old male presents with chest pain.
JAMA Intern Med 2021 Case: A 60-year-old man presents to the emergency department (ED) after his wife found him to be drowsy and confused at home. On arrival to the ED his vitals are normal aside from a decreased level of consciousness and he is found to have a serum sodium concentration of 118 mmol/L.
Background: Patients present commonly to their primary care providers (PCPs) and to the emergency department (ED) with complaints of a sore throat. million visits annually to PCPs and EDs for sore throat. The ibuprofen did not help and he is requesting antibiotics so he can get back to work sooner. In the US, adults accounted for 6.6
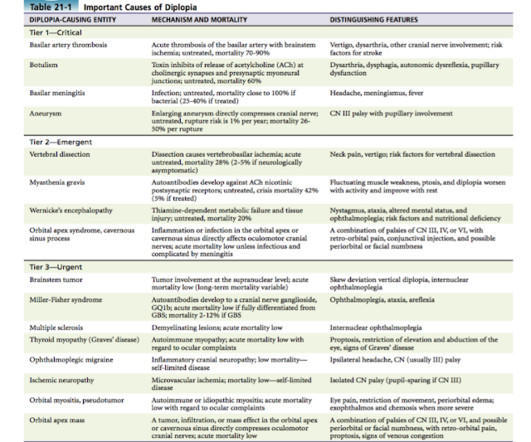
Diplopia is one such complaint which we might come across in ED. Primary eye disorders or systemic diseases presenting as ophthalmologic complaints may present to the Emergency Department especially when symptoms are acute in onset. Key Questions when evaluating diplopia: 1. Is it Monocular or Binocular Diplopia? Associated pain?
AEM October 2022 Guest Skeptic: Dr. Justin Morgenstern is an emergency physician and the creator of the #FOAMed project called First10EM.com Case: A 19-year-old man presents to the emergency department (ED) with his first time anterior should dislocation after trying to recreate one of his favourite scenes in the movie Lethal Weapon.
Background: Patients presenting to emergency departments (EDs) with epigastric pain are typically treated with an antacid, either alone or combined with other medications. There are mixed results from studies with varying methodological quality looking at acute dyspepsia management in the ED. A randomized double-blind clinical trial.
Patients with DRESS syndrome are at risk of developing systemic autoimmune sequelae, which can appear anywhere from months to 4 years after the initial event [1]. In: Nelson L, Howland MA, Lewin NA, Goldfrank LR, Hoffman RS, eds. [1-3] Cutaneous manifestations typically consist of an urticarial, maculopapular eruption.
SGEM#71 : Like a Rolling Kidney Stone (A Systematic Review of Renal Colic) * Bottom Line: Tamsulosin is useless in most ED patients with ureteral colic unless their stone size exceeds at least 4mm. *
First responders found him to be very tachycardic , confused, perserverating and with no memory of the event. First ED ECG is Wellens' (pain free). There was tongue biting. Lightheadedness continued. The tachycardia was gone by the time paramedics arrived. He had a prehospital ECG: What do you think? Interpretation.
Four-year-old Ed is being resuscitated for presumed Invasive Group A Streptococcal Sepsis from tonsilitis. He presented tachycardic and hypotensive with a capillary refill time of 5 seconds. After 40ml/kg of IV 0.9% NaCl, his HR came down a little, but the effect was short-lived. He has an HR of 190/min, and his BP is 85/35 mmHg.
One solution to decrease ICU admission is to treat these patients in the ED until their anion gap is closed and the patient can be transitioned from IV insulin infusion to SQ insulin. The SQuID Protocol (Subcutaneous Insulin in /diabetic Ketoacidosis): Impacts on ED Operational Metrics. Paper: Griffey RT et al. Acad Emerg Med 2023.
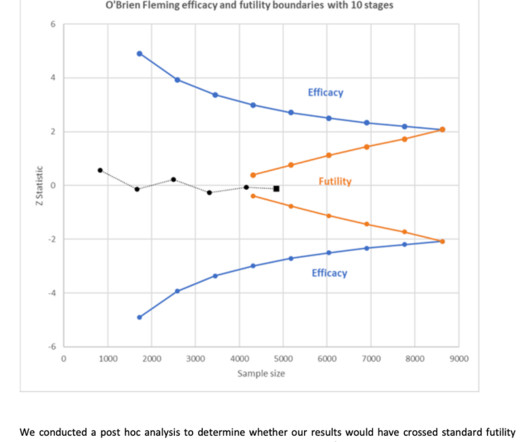
However, the unblinded nature of the trial confounds a bit of interpretation of the influence of the crossover event. These were, effectively, stable-but-not-fully-improved inpatients at a small risk for further deterioration, not the acute respiratory distress seen in the ED. in each group.
Here is the first ED ECG recorded, now pain free after sublingual Nitro: There is what appears to be a reperfusion T-wave in I and aVL. link] = My Comment by K EN G RAUER, MD ( 11/14 /2023 ): = One of the most helpful clinical clues in support that an acute cardiac event is ongoing — is the finding of " dynamic " ECG changes.
As hospital boarding, increased emergency department (ED) volumes, and complexity of patients have increased, so have wait times. 1 When space is limited, patients medical history is rarely protected from the vision or hearing of other patients and guests in the ED. The sensitivity of the details of an ankle sprain may seem minor.
Epinephrine – 10ug/mL, 10mL syringe Phenylephrine – 100ug/mL, 10mL syringe Phenylephrine bolus doses from 100-200ug and epinephrine 10-20ug administered every 2-5 minutes pursuant to provider order Inclusion Criteria: Adults age >18 years old Received at least one bolus dose of phenylephrine or epinephrine pre-filled syringes Exclusion (..)
Case: You are working in the emergency department (ED) and have just been involved in a difficult case in the resuscitation room. He writes a blog called Broken Toy covering topics such as his experience with burnout, medical education and looking after each other. Rudeness does not need to be part of medicine.
KEY POINTS from this CASE: The presenting history often provides invaluable clues to the likelihood of an acute cardiac event. ( This is a "low prevalence" history for an acute cardiac event.). But this measurement was at the J-point, which on this ECG is 4 mm. STE at 60 ms after the J-point is substantially higher than at the J-point.
Two large, cluster-randomized trials ( SMART and SALT-ED ) showed a small benefit to the use of balanced crystalloids in preventing a composite outcome of Major Adverse Kidney Events within 30 days (aka MAKE-30). Since then that debate has broadly centered on the choice between what we will call “abnormal saline” (0.9%
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content