This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Around 6 million people in the U.S. 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. Background Around 6 million people in the U.S. Background Around 6 million people in the U.S.
of people who take NSAIDs ( Nzeako 2010 ). patients that take ACE inhibitors (but 20-30% of all angioedema presentations to the Emergency Department) 3 times more common in Black Americans ( Kostis 2005 ) 0.01 of people who take NSAIDs ( Nzeako 2010 ). Typically involves the mouth, larynx, pharynx, and subglottic tissue ( Kostis 2005 ).
Why is serum calcium important to draw in the ED for the patient who is exsanguinating? If someone is on anti-platelets or anticoagulants what is the best strategy to ensure the docs in the ED know what to give and how much? What should be the lab resuscitation targets? How do we mitigate the risk of hypothermia?
Not so much for the patient but it’s one of those ones that is niche enough to not have been picked up via the usual filters of ED, medical team to the ward. Theoretically giving them FFP while waiting on PLEX seems like it might be sensible but in reality probably does nothing when the autoantibodies are still around.
Case: A 71-year-old man is brought to your emergency department (ED) by emergency medical serviced (EMS) having fallen two steps at home. The transfusion tech calls to remind you that your protocol is currently under review, and asks if would you like the 1:1 or the 1:3 version of fresh-frozen plasma (FFP) to packed red blood cells (pRBC)?
Takeaway lessons * In an ideal world, penetrating abdominal trauma in an unstable patient would proceed directly to the OR with no delay by the ED. Not too much role for TEG in the initial ED presentation. Continue to use a balanced ratio unless you can use TEG to guide FFP and platelets.* FFP is delayed or unavailable; 2.
Most major hemorrhage protocols give a balanced transfusion of PRBCs, FFP, and platelets in ratios approaching concentrations found in whole blood. Fibrinogen and fibrin are often depleted during major trauma as a result of consumption, breakdown, and dilution. Fibrinogen products may also be needed to stabilize clots and stem bleeding.
A 37-year-old G5P4 at 33 weeks presents to the ED after being brought in by ambulance. We’ll keep it short, while you keep that EM brain sharp. She had a precipitous delivery while the ambulance was pulling in. The newborn is doing well, but the mother is complaining of shortness of breath and chest pain.
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. The trauma call goes out. You will be running the show today, and you want to use your preparation time well. The priority is the drain and blood replacement.
Fresh frozen plasma, or FFP, should only be given to cirrhotic patients as part of the massive transfusion protocol in cases of profound hypotension, as “patients with cirrhosis rarely have true enzymatic hypocoagulability, and FFP may worsen bleeding due to over-resuscitation and dilution of coagulation factors.”
FFP and platelets also contain citrate. How does this impact what you do in the ED? A meta-analysis found that 56% of patients with severe trauma resulting in hypotension have hypoCa.There was an increase in mortality, increased need for transfusion, and increased risk of coagulopathy in patients with hypoCa. mmol/L to 1.3
2 TTP often presents abruptly, and most patients that develop it first visit the emergency department (ED) as their symptoms worsen. 1 Pregnant patients are particularly vulnerable to misdiagnosis of TTP in the ED. 1 Pregnant patients are particularly vulnerable to misdiagnosis of TTP in the ED. creatinine less than 2.0
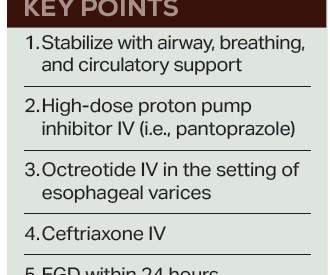
On arrival to the ED the patient’s initial vital signs are temperature 38.5C, BP 102/48, HR 106, RR 20. A partner at bedside reports recent depressed mood, abdominal pain, and vomiting yesterday. The patient woke up confused this morning, and has had a worsening mental status throughout the day today. Be wary of this stage.
Airway: Key decision: base decision for intubation on clinical course, efficacy of airway clearance (coughing, mental status), ED/institutional resources, respiratory status (respiratory failure). Warfarin: vitamin K 10 mg IV and PCC or FFP. Fibrinogen level < 150 mg/dL: cryoprecipitate or fibrinogen concentrate (not FFP).
Ali, a 12-year-old male, is pre-alerted by ambulance to ED. How would you prepare for the patient’s arrival to ED? Do I have emergency blood available in the ED? Trauma is the most significant contributor to childhood mortality, with the mechanism changing with maturity and social development.
ED Evaluation Transport to the ED from the refugee reception center takes 1 hour. Labs Laboratory workup in the ED is notable for a leukocytosis of 41,000/L, hemoglobin of 6.5 The family reports no history of food allergies, insect bites, or contact with sick individuals. The neck is supple with a macular rash present.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content