This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
With emergency department (ED) volumes rising, administrators are eager to explore AI-driven solutions to improve patient safety and reduce staff burnout. They want to know how CHARTWatch integrates with electronic health records (EHRs), whether it can adapt to their patient ED population, and how clinicians respond to using the tool.
He has been involved in ED-based clinical research examining ways to improve care for patients with alcohol use disorder in the ED for over two decades. Case 1: A patient presents to the ED with nausea, vomiting and some abdominal pain complaining of alcohol withdrawal. This is an SGEM HOP but with a twist.
Fever in the Emergency Department Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. Outside his family and work, Jesse pours […] The post SGEM#195: Some Like It Hot – ED Temperature and ICU Survival first appeared on The Skeptics Guide to Emergency Medicine. Critical Care Medicine 2017.
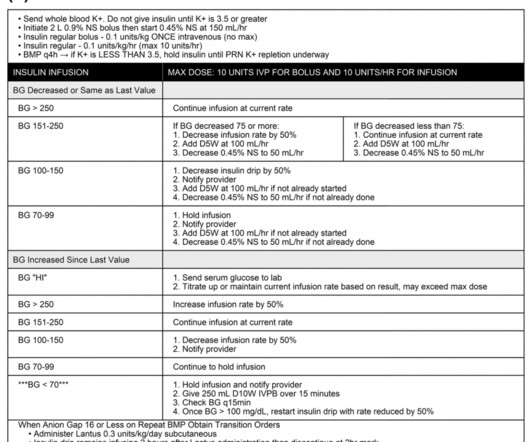
The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” He is otherwise healthy.
The SQuID Protocol (Subcutaneous Insulin in Diabetic Ketoacidosis): Impacts on ED Operational Metrics. The standard of care of treating DKA is fluid resuscitation, electrolyte management, and intravenous insulin infusion in the intensive care unit (ICU) setting for close glucose and electrolyte monitoring. Image from cited article.
Historically, it has been used more frequently in the ICU than in Emergency Departments, likely due to provider comfort. […] The post Is there a Precedence for Precedex in the ED? It offers a unique profile of sedation without respiratory depression, making it an attractive option in various clinical scenarios.
Discussing ICU triage, risk stratification, and patient disposition with intensivist Eddy Joe Gutierrez (@eddyjoemd) of the Saving Lives Podcast. Takeaway lessons * When a patient has borderline indications for requiring the ICU, generally, in the real world, they should go to the ICU.
He is board certified […] The post SGEM#368: Just A Normal Saline Day in the ICU – The PLUS Study first appeared on The Skeptics Guide to Emergency Medicine. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates. .
They were randomized to ceftriaxone 2gm intravenous (IV) in the ambulance or usual cares (fluids and supplementary oxygen) until arrive to the ED. The primary outcome reported was no statistical difference in mortality at 28 days (8% in both groups) despite giving antibiotics 96 minutes earlier [2].
Date: April 25, 2024 Guest Skeptic: Missy Carter is a PA working in an ICU in the Tacoma area and an adjunct faculty member with the Tacoma Community College paramedic program. When emergency department (ED) staff roll her to remove her clothing her humeral intraosseous (IO) is dislodged. Prehospital Emergency Care. February 2024.
Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. There is certainly a need for more practical application for the ED doc or initial setup of patients on the vent.
Are you using phenobarbital instead of benzodiazepines as the first-line monotherapy for patients in alcohol withdrawal in the Emergency Department (ED)? Is phenobarbital safe for the treatment of EtOH withdrawal in the ED? If not, you probably should be. Another old drug for a new indication, right? Well not exactly. In short, yes.
A narrow pulse pressure has been shown to predict the need for hemorrhage control in the ED setting but has not been assessed as a predictor in the prehospital setting. A narrow pulse pressure occurs due to compensatory increased systemic vascular resistance in the setting of decreased cardiac output.
Our experience: Traditionally, ED physicians do not like ordering urine drug screens (UDS). We have certainly seen patients who have pain which is controlled and still have psychomotor agitation and sympathetic activation, leading some to require ICU admission for dexmedetomidine and/or ketamine infusion. JAMA Network Open.
REBEL Cast Ep120: Etomidate vs Ketamine for RSI in the ED? PMID: Clinical Question: Does a single dose of ketamine or etomidate used for rapid sequence intubation (RSI) of critically adults in the ED impact the SOFA score within 3 days of hospitalization? Click here for Direct Download of the Podcast Paper: Knack SKS et al.
Case: It’s another day, another dollar in the emergency department (ED). You wonder if she could have an allergy challenge dose of ceftriaxone in the ED. Emergency Physicians frequently encounter ED patients with self-reported penicillin allergies. AEM August 2024. The next patient is a 63-year-old woman with a cough and fever.
It is unacceptable to have the rates of Awareness during Paralysis seen in a recent ED sedation study--We are better than this. EMCrit Project by Scott Weingart, MD FCCM.
European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED.
Mild to moderate DKA represents a subgroup of patients that often require admission to the ICU due to hospital policies not allowing insulin infusions outside of this clinical setting. The SQuID Protocol (Subcutaneous Insulin in /diabetic Ketoacidosis): Impacts on ED Operational Metrics. Paper: Griffey RT et al. Acad Emerg Med 2023.
Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Reference: Cashen K, Reeder RW, Ahmed T, et al. Pediatric Crit Care Med.
For example a pt in the ED with sepsis, and a collapsible IVC, dry lungs and no peripheral edema is more likely to benefit from fluid than be harmed Take that same pt, with the same US and physical exam findings and make it 72-hrs later in the ICU after 6-10 L. For this we use clinical judgement, US findings, PE findings.
40 year old healthy ICU nurse, works with COVID-19 patients. She was brought to ED by ambulance after collapsing in a shower. Her pulse rate was 120 and blood pressure was 120/80. Her blood gases (…
. #1: PREOXI RCT – Preoxygenation with Noninvasive Ventilation vs. Non-rebreather Mask Spoon Feed Noninvasive ventilation (NIV) was superior to a standard non-rebreather (NRB) oxygen mask for preoxygenation of critically ill ED or ICU patients requiring intubation, with a NNT of 11 to prevent 1 episode of hypoxemia <85%.
Spoon Feed Advanced statistics emulating clinical trial protocols from an ICU database did not identify consistent differences in 30-day mortality when ICU patients were intubated early (within 8 hours of admission) or late (after 48 hours). Clay Smith at @spoonfedEM , and sign up for email updates here. #1: Neurology vol.
Looking at the workflow of a fresh post-op open heart surgery patient, as well as what to do when it devolves into cardiac tamponade, with (returning) guest Brendan Riordan, cardiothoracic ICU PA (@concernecus) at the University of Washington, and his NP colleague Kris Ramilo (@krsrml0). Audio quality was a bit dodgy in this one; sorry all!–eds.]
I was about two months into a family practice internship when I went to visit my uncle whose neighbor happened to be an ED resident, Dr. Clarke said. ED attendings Dr. Gerald Whelan and Dr. Shumary Chow supervising a full arrest in C booththe main trauma roomwith an ED tech administering CPR. Click to enlarge.) Click to enlarge.)
Max is then going to Georgetown to be an attending in both EM and ICU. Case: It’s another day in your emergency department (ED). The triage nurse places a 61 year-old-man with fever, hypotension, cough into the smallest room in the ED. You scan through the EMR and see the blood pressure is 60/40.
2020 Case: A 74-year-old woman who suffered a fall earlier today presents to the emergency department (ED) and is found to have five rib fractures to her right thorax, but no other injury. His team found grip strength was weakly correlated with frailty in older ED patients [6]. J Trauma Acute Care Surg. Reference: Schuster et al.
Our guest is trauma surgeon Dr. Dennis Kim ( @traumaicurounds ), associate professor of Clinical Surgery at UCLA and medical director of the Harbor-UCLA Medical Center SICU, as well as host of the Trauma ICU Rounds podcast. Traction splinting is usually not done in the ED.
Intravenous insulin infusions typically require treatment in highly monitored settings, such as an intensive care unit (ICU) or step-down unit for safety and due to the frequency and intensity of monitoring. ICU and step-down beds are a limited resource and generate higher hospital charges. JAMA Netw Open. 2022;5(4):e226417.
. #1: DEVICE RCT – VL vs DL for Critically Ill Adults Spoon Feed Video laryngoscopy (VL) was associated with higher rates of first attempt intubation success compared to direct laryngoscopy (DL) for critically ill patients in the ICU and ED.
2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Over the past few years, there has been an increase in emergency department (ED) volumes and lengths of stay. The typical nursing to patient ratio is 1:3 with a shared respiratory therapist for the entire ED.
Case: A 59-year-old woman comes is brought into your emergency department (ED) by EMS in cardiac arrest. The patient achieved return of spontaneous circulation (ROSC) on arrival to the ED. She had a witnessed arrest, and CPR was initiated by bystanders.
University of Maryland Department of Emergency Med
JULY 17, 2023
Central Venous Catheter (CVC; aka central line) placement is a common procedure in both the ED and ICU, and while overall quite safe, does ca. Click to view the rest
You are on-call – covering medicine and ICU admissions – while overseeing 20 admitted patients. You receive 3 new admissions from the ED, but you still have to move 2 sick patients to the ICU. Your wards are at capacity. You also have to prepare 3 discharges for the next morning.
PMID: 38592662 Bottom line: Would you be happy if you kid follow-ed your footsteps into emergency medicine? For the most part, central lines can be left to the ICU team during day time hours (and a good percentage of patients will never need one). Maybe ED is not the best place for all patients! 2024 Jun;26(6):381-385.
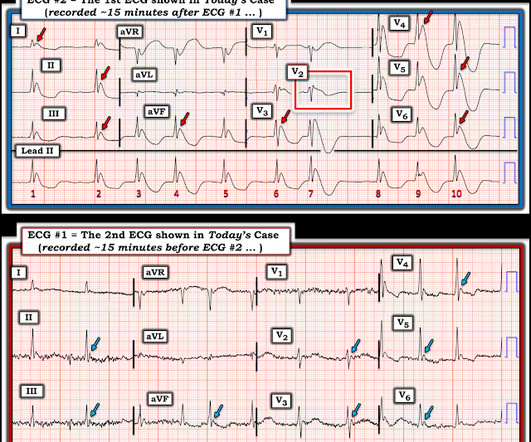
A 65 y/o Female was admitted to the ICU for septic shock. The combination of prolonged QT and deep T wave inversion throughout the precordium is typical of Takotsubo syndrome, or Stress Cardiomyopathy – which can occur in the context of a physiologically distressed ICU patient, further compromising their hemodynamics. Surawicz, B.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Propofol utilized for sedation; patient admitted to ICU for EEG monitoring. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. They administer two doses of 10 mg midazolam IM.
He was intubated on arrival at the ED for mental status and airway protection due to vomiting. His temperature was brought back to normal over time in the ICU. There is also large T wave inversion and long QT. Clinical context: A man in his 50s was found down outside in the cold, unresponsive but with intact vital signs.
These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. Hemodynamics slowly begin to stabilize, and the patient is transferred to the ICU for further post-cardiac arrest care. doi:10.1007/BF03161199 Olson K, Smollin C, eds.
Everyone on the team from the pre-hospital setting, to the ED, in-patient, ICU and primary care providers. I can’t tell you how much it means to have an audience of people committed to providing patients with great care in their time of need. Take a moment to recognize what an important role you play in so many lives.
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content