This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
With emergency department (ED) volumes rising, administrators are eager to explore AI-driven solutions to improve patient safety and reduce staff burnout. They want to know how CHARTWatch integrates with electronic health records (EHRs), whether it can adapt to their patient ED population, and how clinicians respond to using the tool.
fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold fold higher risk of NSTI than the control group 12 For those without comorbidities , AUD exhibited a 15.2-fold
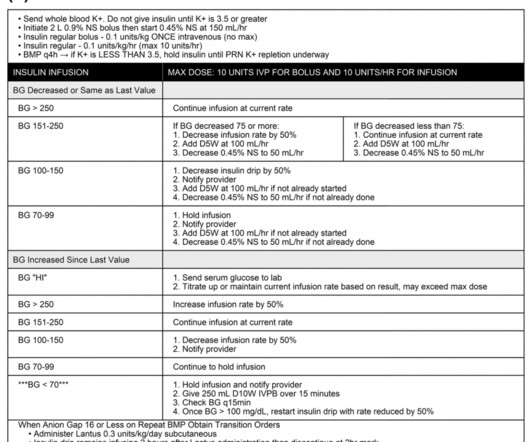
The SQuID Protocol (Subcutaneous Insulin in Diabetic Ketoacidosis): Impacts on ED Operational Metrics. The standard of care of treating DKA is fluid resuscitation, electrolyte management, and intravenous insulin infusion in the intensive care unit (ICU) setting for close glucose and electrolyte monitoring. Image from cited article.
The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. The SQuID protocol (subcutaneous insulin in diabetic ketoacidosis): Impacts on ED operational metrics. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” He is otherwise healthy.
He is board certified […] The post SGEM#368: Just A Normal Saline Day in the ICU – The PLUS Study first appeared on The Skeptics Guide to Emergency Medicine. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates.
Discussing ICU triage, risk stratification, and patient disposition with intensivist Eddy Joe Gutierrez (@eddyjoemd) of the Saving Lives Podcast. Takeaway lessons * When a patient has borderline indications for requiring the ICU, generally, in the real world, they should go to the ICU.
Background: The immediate post intubation period in the ED is a critical time for continued patient stabilization. The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. Short acting.
They were randomized to ceftriaxone 2gm intravenous (IV) in the ambulance or usual cares (fluids and supplementary oxygen) until arrive to the ED. The primary outcome reported was no statistical difference in mortality at 28 days (8% in both groups) despite giving antibiotics 96 minutes earlier [2].
Some bench work, observational studies, and now two large, unblinded, cluster-randomized single-center trials ( SMART and SALT-ED ) suggested a benefit to using balanced crystalloids (i.e. The SALT-ED trial was also a single-centre unblinded trial, but the primary outcome was hospital free days. Reference: Zampieri et al.
Date: April 25, 2024 Guest Skeptic: Missy Carter is a PA working in an ICU in the Tacoma area and an adjunct faculty member with the Tacoma Community College paramedic program. When emergency department (ED) staff roll her to remove her clothing her humeral intraosseous (IO) is dislodged. Prehospital Emergency Care. February 2024.
Are you using phenobarbital instead of benzodiazepines as the first-line monotherapy for patients in alcohol withdrawal in the Emergency Department (ED)? Is phenobarbital safe for the treatment of EtOH withdrawal in the ED? If not, you probably should be. Another old drug for a new indication, right? Well not exactly. In short, yes.
Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. There is certainly a need for more practical application for the ED doc or initial setup of patients on the vent.
A narrow pulse pressure has been shown to predict the need for hemorrhage control in the ED setting but has not been assessed as a predictor in the prehospital setting. A narrow pulse pressure occurs due to compensatory increased systemic vascular resistance in the setting of decreased cardiac output.
European Journal of Internal Medicine , [link] You can listen to my 27-minute rant on Youtube here: [link] This multinational trial looked at a three-pronged diagnostic protocol in the ED for adults with suspected acute aortic syndromes. The protocol used the ADD score, a POCUS echo protocol and D-dimer to try and exclude AAS in the ED.
Background: Patients with decreased level of consciousness due to alcohol, drugs, or medications commonly present to the ED. These patients can be at risk of vomiting and aspiration and often prompts clinicians to pursue definitive airway management to avoid pneumonia and other complications.
More than 1/3 of geriatric trauma patients presenting to the ED after a fall return to the ED or die within one year of initial evaluation. 4 Elderly patients, who comprise only 8-12% of total ED major trauma cases, represent a disproportionate 15-30% of trauma mortalities and costs. Perdue &al. Am J Emerg Med. Liu &al.
Case: It’s another day, another dollar in the emergency department (ED). You wonder if she could have an allergy challenge dose of ceftriaxone in the ED. Emergency Physicians frequently encounter ED patients with self-reported penicillin allergies. AEM August 2024. The next patient is a 63-year-old woman with a cough and fever.
REBEL Cast Ep120: Etomidate vs Ketamine for RSI in the ED? PMID: Clinical Question: Does a single dose of ketamine or etomidate used for rapid sequence intubation (RSI) of critically adults in the ED impact the SOFA score within 3 days of hospitalization? Click here for Direct Download of the Podcast Paper: Knack SKS et al.
For example a pt in the ED with sepsis, and a collapsible IVC, dry lungs and no peripheral edema is more likely to benefit from fluid than be harmed Take that same pt, with the same US and physical exam findings and make it 72-hrs later in the ICU after 6-10 L. That is a holy grail that we have to stop chasing.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Reference: Cashen K, Reeder RW, Ahmed T, et al. Pediatric Crit Care Med.
Dr. Anireddy Reddy Case: A 3-year-old girl presents to the emergency department (ED) with fever and respiratory distress. Your ED team quickly intubates her and places her on a ventilator. Her parents tell you that she has been sick for almost a week and her symptoms seem to be getting worse. Her oxygen saturation is 78% on room air.
Mild to moderate DKA represents a subgroup of patients that often require admission to the ICU due to hospital policies not allowing insulin infusions outside of this clinical setting. The SQuID Protocol (Subcutaneous Insulin in /diabetic Ketoacidosis): Impacts on ED Operational Metrics. Paper: Griffey RT et al. Acad Emerg Med 2023.
Case: A 14-month-old boy presents to the emergency department (ED) with two days of upper respiratory symptoms and respiratory distress. Previous research has shown that HFNC can lower the rate of escalation of care but showed no impact on admission to the intensive care unit (ICU) or length of stay [1]. He has a cough, fever of 38.5°C,
Takeaway lessons Many decisions in the ED are less about what to do, and more about when to do it. Takeaway lessons * Many decisions in the ED are less about what to do, and more about when to do it. Goals of care starts in the ED, and not with lip service. ICU time and ED time are different.
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. I interpreted this tracing knowing only that the patient was a woman in her 60s, with a prior history of proximal LAD OMI — who now presented to the ED with a history of new chest discomfort and shortness of breath.
The ED clinician should inquire about a relevant history of HIV infection, malignancy, high-dose corticosteroid use, chemotherapy, organ transplant, or use of immunosuppressive drugs for other indications. She reports occasional central chest pain exacerbated by coughing. 0 C, and has no jaundice. of PJP patients with sensitivity of 86.5%
I was about two months into a family practice internship when I went to visit my uncle whose neighbor happened to be an ED resident, Dr. Clarke said. ED attendings Dr. Gerald Whelan and Dr. Shumary Chow supervising a full arrest in C booththe main trauma roomwith an ED tech administering CPR. Click to enlarge.)
1: PREOXI RCT – Preoxygenation with Noninvasive Ventilation vs. Non-rebreather Mask Spoon Feed Noninvasive ventilation (NIV) was superior to a standard non-rebreather (NRB) oxygen mask for preoxygenation of critically ill ED or ICU patients requiring intubation, with a NNT of 11 to prevent 1 episode of hypoxemia <85%.
Looking at the workflow of a fresh post-op open heart surgery patient, as well as what to do when it devolves into cardiac tamponade, with (returning) guest Brendan Riordan, cardiothoracic ICU PA (@concernecus) at the University of Washington, and his NP colleague Kris Ramilo (@krsrml0). Audio quality was a bit dodgy in this one; sorry all!–eds.]
REBEL Cast Ep119: A Discussion with Scott Weingart on the CT FIRST Trial Click here for Direct Download of the Podcast Timing Is 6hrs reasonable because most pts excluded because of this Right before heading up to ICU seems good 1st couple hours after ROSC…pts are high risk for re-coding Where Not single coverage or stand-alone EDs Optimize and transfer…scans (..)
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk.
2020 Case: A 74-year-old woman who suffered a fall earlier today presents to the emergency department (ED) and is found to have five rib fractures to her right thorax, but no other injury. His team found grip strength was weakly correlated with frailty in older ED patients [6]. J Trauma Acute Care Surg. Reference: Schuster et al.
Case: A 59-year-old woman presents to the emergency department (ED) with fever, tachycardia, and hypotension. She is admitted to the intensive care unit (ICU) for septic shock. The ICU team is considering using Vitamin C therapy for this patient. She is found to have a urinary tract infection. Reference: Lamontagne F et al.
Question: In adult patients admitted to the ICU with severe CAP, does hydrocortisone compared to placebo reduce 28-day all-cause mortality? Question: In adult patients admitted to the ICU with severe CAP, does methylprednisolone compared to placebo reduce 60-day all-cause? Reyes LF, Garcia E, Ibáñez-Prada ED, et al.
Dennis Kim ( @traumaicurounds ), associate professor of Clinical Surgery at UCLA and medical director of the Harbor-UCLA Medical Center SICU, as well as host of the Trauma ICU Rounds podcast. Likewise, many penetrating injury patients with palpable pulses can wait for further resuscitation (whether blood or anything else) until surgery.
Spoon Feed Advanced statistics emulating clinical trial protocols from an ICU database did not identify consistent differences in 30-day mortality when ICU patients were intubated early (within 8 hours of admission) or late (after 48 hours). Originally published at JournalFeed , a site that provides daily or weekly literature updates.
A 37-year-old G5P4 at 33 weeks presents to the ED after being brought in by ambulance. We’ll keep it short, while you keep that EM brain sharp. She had a precipitous delivery while the ambulance was pulling in. The newborn is doing well, but the mother is complaining of shortness of breath and chest pain.
Intravenous insulin infusions typically require treatment in highly monitored settings, such as an intensive care unit (ICU) or step-down unit for safety and due to the frequency and intensity of monitoring. ICU and step-down beds are a limited resource and generate higher hospital charges. glargine 0.3 JAMA Netw Open. Acad Emerg Med.
This is critical for the EMS provider, or ED clinician, as identification of Grade I ischemia (aka, HATW’s) addresses the culprit lesion at the earliest opportunity with excellent downstream prognosis for the patient. [2] The following ECG was captured upon arrival at the receiving ED. The ED resulted an 8.7 An ECG is recorded.
They consecutively enrolled 1,817 ICU patients from 45 sites across China. Population: Inclusion Criteria: Age 18-75 years old SOFA score 2-13 Admitted to the ICU with a diagnosis of sepsis 3.0, “ Life-threatening organ dysfunction caused by a dysregulated host response to infection.” 002) ICU-free days: Placebo 12.4%
It wasn’t until over 20 minutes later that they managed to secure an airway and transfer her to the ICU, where she died 13 days later. Having just completed my Paediatric ED placement, I donned the navy flight suit and spent two weeks learning how to deal with every conceivable le in-flight emergency.
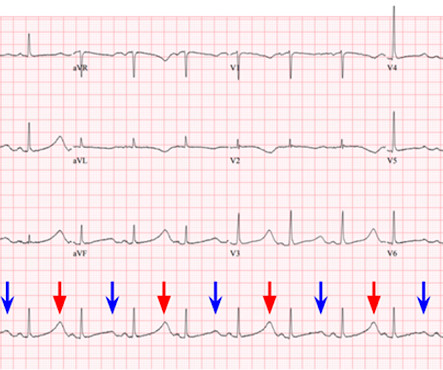
On arrival to the ED the patient was intubated with normal vital signs. She was admitted to the ICU where subsequent ECGs were performed: ECG at 12 hours QTc prolongation, resolution of T wave alternans ECG at 24 hours Sinus tachycardia with normalized QTc interval. No ischemic ST changes.
A 65 y/o Female was admitted to the ICU for septic shock. The combination of prolonged QT and deep T wave inversion throughout the precordium is typical of Takotsubo syndrome, or Stress Cardiomyopathy – which can occur in the context of a physiologically distressed ICU patient, further compromising their hemodynamics.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content