This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
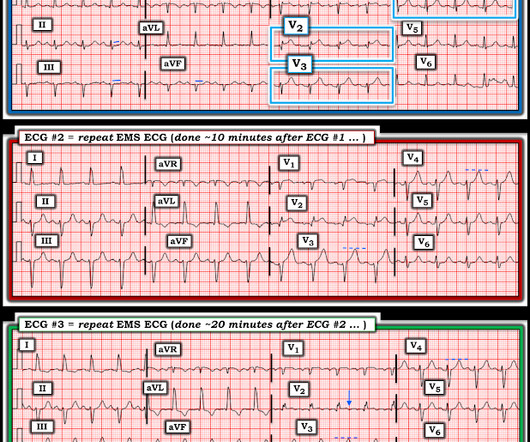
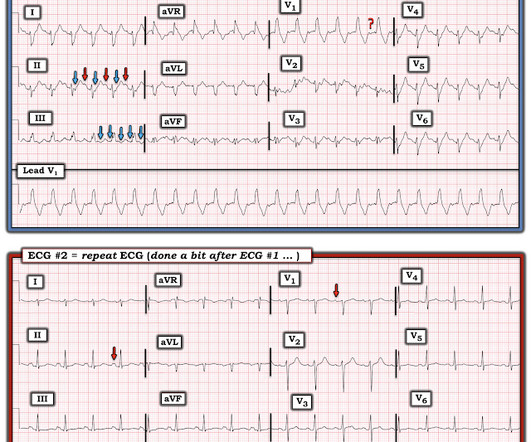
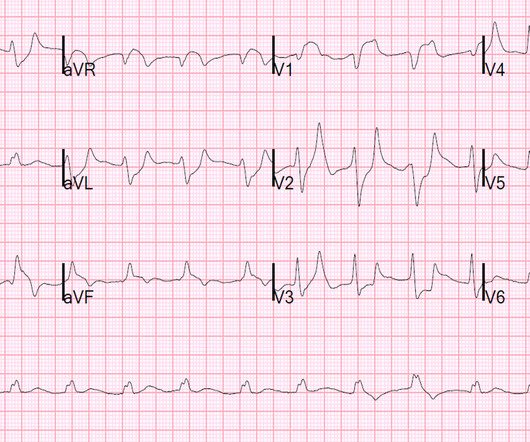
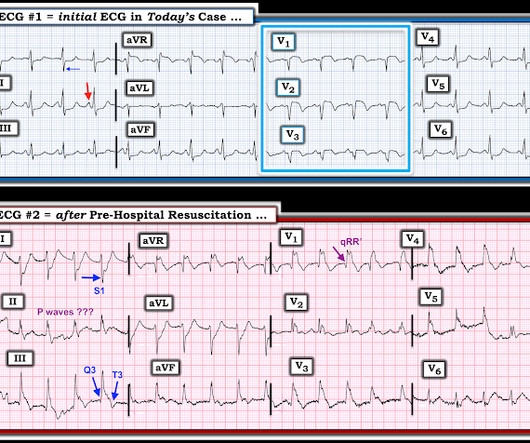
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
He arrived to the ED with severe hypotension, heart rate in the 70s, unable to follow commands but moving all extremities requiring restraint and sedation, respiratory rate around 24/min being supported with bag valve mask, with significant hypoxemia. Further information is not available.
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. I sent both ECGs to Dr. Smith, with the only information that these were prior vs new ECG. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient.
Sent by anonymous, written by Pendell Meyers I received a text with this image and no other information: What do you think? The interventional cardiologist then canceled the activation and returned the patient to the ED without doing an angiogram ("Not a STEMI"). I simply texted back: "Definite posterior OMI."
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. The Queen gets it right First ED ECG: Hyperacute T-waves persist.
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
He has a history of STEMI and heart failure. I read this blinded, with no clinical information, and read it as inferior OMI. The Queen of Hearts interprets it blinded also (no clinical information and no previous ECGs or serial ECGs). link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics.
This case was recently posted by Tyron Maartens on Facebook EKG club (he agreed to let me post it here), with the following clinical information: "42 year old male with two weeks of intermittent chest discomfort, awoke 4 hours prior to this ECG with a more severe, heavy chest pain (5/10). Both support acute anterior STEMI. 3.0 = 0.50
Here is his initial ED ECG: What do you think? Any ST Depression Maximal in V1-V4 is OMI until proven otherwise I sent this ECG with no information to Pendell. Here it is: Obvious Inferior Posterior STEMI (+) OMI. Then the ED doc would be dependent on that first ECG. We send each other EKG by the dozens every day.
Jason was very skeptical of STEMI. This also argues against STEMI. Unfortunately, this option might not be available for pre-hospital tracings ( but it can be done once the patient arrives in the ED for their initial hospital tracing ). He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree.
The ECG shows an inferior ST-Elevated Myocardial Infarction (STEMI). They felt this would help inform guideline writers on making recommendations in this area. His vitals are: heart rate of 72 beats per minute, blood pressure of 150/90, respiratory rate of 14 breaths per minute and oxygen saturation of 93%. Class IIb, LOE C-LD)
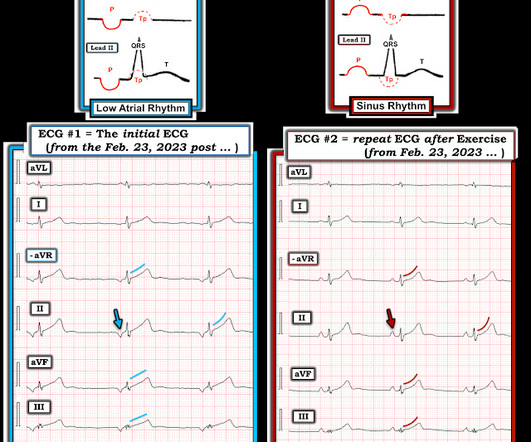
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. Triage ECG: What do you think?
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
The neighbor recorded a systolic blood pressure again above 200 mm Hg and advised her to come to the ED to address her symptoms. Recall from this post referencing this study that "reciprocal STD in aVL is highly sensitive for inferior OMI (far better than STEMI criteria) and excludes pericarditis, but is not specific for OMI."
The chest pain started about 24 hours ago, but there was no detailed information available about whether his pain had come and gone, or what prompted him to be evaluated 24 hours after onset. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Learning Points: 1.
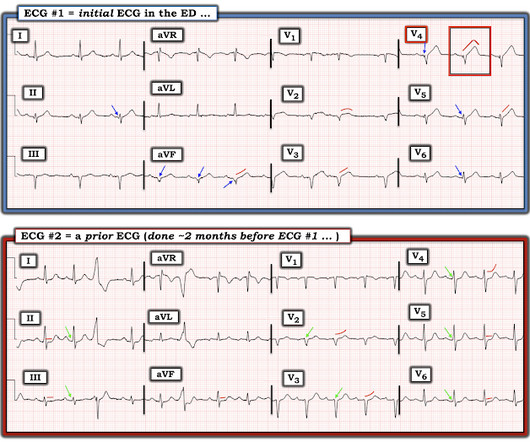
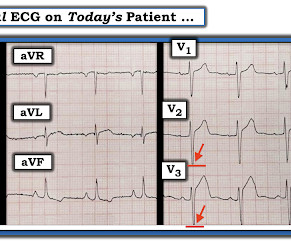
== MY Comment , by K EN G RAUER, MD ( 8/30 /2024 ): == I was sent the ECG shown in Figure-1 — knowing only that the patient was being seen in the ED ( E mergency D epartment ). 2 Informational: I was provided with a repeat ECG on this patient — which was recorded a bit after ECG #1, still in the ED ( Bottom tracing in Figure-3 ). . #2
Are Some Cardiologists Really Limited by Strict Adherence to STEMI millimeter criteria? I was texted these ECGs by a recent residency graduate after they had all been recorded, along with the following clinical information: A 50-something with no cardiac history, but with h/o Diabetes, was doing physical work when he collapsed.
He reports that this chest pain feels different than prior chest pain when he had his STEMI/OMI, but is unable to further describe chest pain. I sent it to 5 of my OMI friends without any clinical information or outcome and all 5 independently responded with exactly the same diagnosis: "reperfused inferior OMI".
[link] Case continued She arrived in the ED and here is the first ED ECG. Optical coherence tomography, due to its high resolution, may provide additional information [ 10,13 ]. This has resulted in an under-representation of STEMI MINOCA patients in the literature. I don't know if her pain was getting better or not.
Written by Jesse McLaren Two patients in their 70s presented to the ED with chest pain and RBBB. The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. Do either, both, or neither have occlusion MI? Vitals were normal.
He sent it to me with no other information and I wrote back "100% diagnostic of LBBB with inferior-posterior-lateral OMI" There is atrial paced rhythm with Left Bundle Branch Block (LBBB). Most large STEMI have peak troponin I in the 20.0 This ECG was recorded and was reviewed remotely by a cardiologist: What do you think?
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern.
EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0
I texted this ECG with no information to Dr. Smith, who immediately said: "If CP, then anterior OMI until proven otherwise." Post Cath ECG: Obviously completing MI with LVA morphology, and STE that meets STEMI criteria (but pt is still diagnosed as "NSTEMI"). Setting – large, academic, suburban ED.
As for precordial leads: this is from my files and I don't have all the information, but it is clearly a right sided ECG (QRS in V5, V6 is inverted from QRS in I, aVL) What else do you see? The cath lab was activated for STEMI. So, in retrospect, the first patient probably did not have STEMI at all. There was no MI. Lessons : 1.
Case An 82 year old man with a history of hypertension presented to the ED with chest pain at 1211. The ED provider ordered a coronary CT scan to assess the patient for CAD. His pain suddenly became much worse in the ED and he became acutely diaphoretic, dizzy, and hypotensive. There is pericardial tamponade.
But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. But the ECG still doesn’t meet STEMI criteria. It was therefore interpreted as “no STEMI” and the patient was treated with dual anti-platelets and referred to cardiology as “NSTEMI.” the cardiologist 5.
Here is his ED ECG There is RV Pacing. is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. is very specific for STEMI , and there is some evidence, as well as rationale, that a paced rhythm behaves similarly. Here is one case of anterior STEMI in a paced rhythm.
If this EKG were handed to you to screen from triage without any clinical information, what would you think? for those of you who do not do Emergency Medicine, ECGs are handed to us without any clinical context) The ECG was read simply as "No STEMI." What do you think? I maintain that this written RR may or may not be accurate.
He still had active pain on arrival to the ED. This morphology can be cause by or associated with cocaine: A Patient with Cocaine Chest Pain and Prehospital Computer interpretation of STEMI This is OMI of the anterior, lateral, and inferior walls until proven otherwise. His initial ECG in the ED ( = E CG # 1 ) is shown in Figure-1.
Dr. Singer sent this to me with just the information: "~40 year old with acute chest pain". Here is the Queen of Heart's interpretation: The cath lab had been activated for concern of STEMI. Other outcome information is not available. Here is his triage ECG: What do you think? I immediately responded: "cool fake!
I want all to know that, with the right mind preparation, and the use of the early repol/LAD occlusion formula, extremely subtle coronary occlusion can be detected prospectively, with no other information than the ECG. This was my thought: if this patient presented to the ED with chest pain, then this is an LAD occlusion. Asymmetric.
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. In STEMI, they are generally upright and large in proportion to the QRS.
The patient arrived in the ED and had this ECG: No difference. Is this an anterior STEMI with LBBB? Explanation : The patient had a worrisome history: 59 yo with significant substernal chest pressure, so his pretest probability of MI (and even of STEMI) is reasonably high. If projected, they are indeed very deep.
This meets "STEMI criteria" However, there is very high voltage, with a very deep S-wave in V2 and tall R-wave in V4. The morphology is not right for STEMI. My interpretation: LVH with secondary ST-T abnormalities, exaggerated by stress, not a STEMI. I did not have more information at the time.
I was reviewing ECGs for a study, and came across this one, and was able to get all the clinical information: What do you think? She was diagnosed with a Non-STEMI and kept overnight for a next day angiogram. Medics recorded the above ECG and called a STEMI alert. Her troponin I returned at 900 ng/L.
There’s mild inferior ST elevation in III that doesn’t meet STEMI criteria, but it’s associated with ST depression in aVL and V2 that makes it diagnostic of infero-posterior Occlusion MI (from either RCA or circumflex)– accompanied by inferior Q waves of unknown age. Are there any signs of occlusion or reperfusion?
Jason was very skeptical of STEMI. This also argues against STEMI. Look for old ECGs Do serial ECGs Do echocardiography June 17, 2016 Anterior STEMI? Unfortunately, this option might not be available for pre-hospital tracings ( but it can be done once the patient arrives in the ED for their initial hospital tracing ).
Submitted by Benjamin Garbus, MD with edits by Bracey, Meyers, and Smith A man in his early 30s presented to the ED with chest pain described as an “explosion" of left chest pressure. At the time of arrival to the ED, the patient reported 1/10 chest pain with normal vital signs. Triage EKG: What do you think? Do NOT use them.
When I was given this case — I initially saw only ECG #1 — and I had not been given any clinical information. How would YOU interpret ECG #1 if this was the only tracing you saw — and — the only thing you knew about the patient, was that he/she was being seen in the ED? MORE Information is Provided!
EMS recorded these ECGs: Time 0: In V2-V4, there is ST elevation that does not meet STEMI "criteria," of 1.5 The patient arrived in the ED. The pain completely resolved after nitroglycerine Moments later, the this ECG was recorded in the ED when she had been pain free for moments only: Computer read: Normal ECG. She called 911.
At this point, with the information above, the patient's overall clinical picture could be consistent with either reperfused OMI, or Non-OMI, since both may have absent pain and inverted T waves. Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI. Transient STEMI is at high risk of re-occlusion.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content