This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
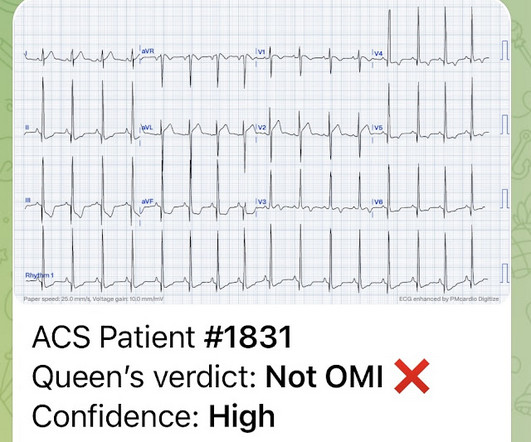
This 29 year old African American patient was found down, unconscious, not breathing and was given 2 mg of intranasal naloxone by a bystander. On arrival to the ED, the patient was diaphoretic, tachycardic. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? and had dilated pupils.
In the field, he was given 4 mg intranasal (IN) naloxone and rescue breaths via bag valve mask. In the ED, he develops recurrent respiratory depression and hypoxia to 80%. He is administered 2mg intravenous (IV) naloxone and shortly after develops precipitated withdrawal with altered mental status, diaphoresis, vomiting, and diarrhea.
SCD, therefore, is not only a mechanical disease but there are also many other cellular and plasma factors as well as endothelial interaction that generate chronic inflammation. Haematology specialist clinics are key to manage the chronic side of the disease, while ED doctors should be able to act rapidly on the common acute emergencies.
A 33-year-old male with a history of drug use presented to the emergency department (ED) for extreme agitation after receiving two doses of 2 mg naloxone by EMS for respiratory depression. If available, an in-house ED pharmacist is an incredible resource for guidance when there are questions regarding pharmacologic management.
While this guide isnt exhaustive, its designed by residents, for residents, to provide practical tips and foundational knowledge thats crucial in the fast-paced, high-stakes environment of the ED. Introduction Airway management is a critical ED skill to master. Figure 7: (modified from Tanoubi 2009).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content