This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. We looked at 101 STEMI patients from two rural EDs. Date: November 22, 2023 Reference: Stopyra et al.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. He arrived to the ED by helicopter at 1507, about three hours after the start of his chest pain while chopping wood around noon. He wrote most of it and I (Smith) edited.
The paramedic called the EM physician ahead of arrival and discussed the case and ECGs, and both agreed upon activating "Code STEMI" (even though of course it is not STEMI by definition), so that the acute LAD occlusion could be treated as fast as possible. So the cath lab was activated. Long term outcome is unavailable.
He called EMS who brought him to the ED. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. ED Diagnoses: 1.
Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." What do you think?
Our data corroborate that immediate management of a patient with a normal automated triage ECG reading is not modified by real-time ED physician ECG interpretation." Smith comment: we showed that the first troponin, even in full-blown STEMI, is negative 25% of the time. But according to Langlois-Carbonneau et al.,
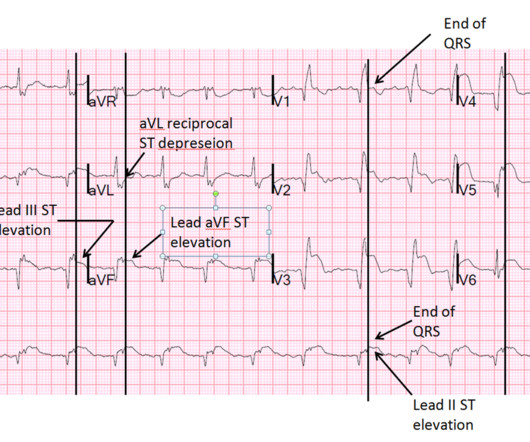
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
While in the ED, patient developed acute dyspnea while at rest, initially not associated with chest pain. The patient had no chest symptoms until he had been in the ED for many hours and had been undergoing management of his DKA. The patient was under the care of another ED physician. Another ECG was recorded: What do you think?
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
male presents to the ED at 6:45 AM with left sided chest dull pressure that woke him up from sleep at 3am. He arrived to the ED at around 6:45am, and stated the pain has persisted. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. The pain radiated to both shoulders.
Jason was very skeptical of STEMI. This also argues against STEMI. Unfortunately, this option might not be available for pre-hospital tracings ( but it can be done once the patient arrives in the ED for their initial hospital tracing ). He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree.
The ST changes went overlooked by both the ED physician and the on-call cardiologist, and the patient was subsequently admitted to telemetry. it has been subsequently deemed a STEMI-equivalent. There was no obvious pallor, diaphoresis, or dyspnea, and he denied any prior episodes of vomiting. However, when the Troponin I returned 8.4
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
He arrived to the ED with severe hypotension, heart rate in the 70s, unable to follow commands but moving all extremities requiring restraint and sedation, respiratory rate around 24/min being supported with bag valve mask, with significant hypoxemia. His family started CPR and called EMS, who arrived to find him in ventricular fibrillation.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Edited by Smith He also sent me this great case. The undergraduate's analysis: This EKG shows J point elevation of about 0.5-1
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] Written by Jesse McLaren Four patients presented with chest pain. have published a number of warnings about the previous reassuring studies.[4,5]
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. The essential "immediate" decision to be made in "zero time" in the ED, is whether or not prompt cath and reperfusion is needed. Could this false positive cath lab activation been prevented?
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. It’s unclear if the paramedic ECGs were seen or missed in the ED. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. At this point the emergency physician asked for a stat cardiology consult.
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Having severe pain drives people to the ED for faster treatment! Which had the more severe chest pain at the time of the ECG?
With a new protocol and Pulsara, Metropolitan Emergency Medical Services can now transport eligible pediatric behavioral health patients directly to behavioral health facilities—resulting in a 44% decrease of pediatric behavioral health patients transported to the ED. MEMS transports around 77,000 patients each year.
On ED arrival GCS is 3, there are rapid eye movements to the right but no other apparent seizure activity. Official diagnosis requires EEG, which is not something we can typically obtain in the ED. After second dose the tonic clonic movement stop; GCS is 3, and she’s unresponsive. NCSE is likely more common than we think.
It is unclear what changes happened to the rhythm based on the EMS interventions, but the patient arrived to the ED remaining critically ill and with a very wide complex reported (no ECGs from ED available sadly). The QRS is so wide and sinusoidal that the only real possibilities left are hyperkalemia or Na channel blockade.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). She arrives in the emergency department (ED) with decreased level of consciousness and shock.
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
George Mastoras (Twitter @georgemastoras), written by Jesse McLaren It’s a busy day in the ED when you’re sent another ECG to sign off from a patient at triage. A healthy 45-year-old female presented with chest pain, with normal vitals. The computer interpretation was “ST elevation, consider early repolarization, pericarditis or injury.”
BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. The patient continued to verbalize cessation of symptoms while in the ED.
The attending crews were concerned for SVT with corresponding ischemic hyperacute T waves (HATW) and subsequently activated STEMI pre-hospital. The following ECG was captured upon arrival at the receiving ED. The ED resulted an 8.7 Then, three minutes later… Crews activated STEMI as she deteriorated into PEA arrest.
Here is his initial ED ECG: What do you think? Here it is: Obvious Inferior Posterior STEMI (+) OMI. Then the ED doc would be dependent on that first ECG. Initial troponin was: 3 ng/L We showed that the first troponin in acute STEMI is often negative in at least 27%. We send each other EKG by the dozens every day.
Here was his initial ED ECG: Formal interpretation by interventional cardiologist: There is "Non-diagnostic" ST Elevation in V2-V4 and aVL. COACT: The COACT trial was fatally flawed, and because of it, many cardiologists are convinced that if there are no STEMI criteria, the patient does not need to go to the cath lab.
Sent by anonymous, written by Pendell Meyers, reviewed by Smith and Grauer A man in his 40s presented to the ED with HTN, DM, and smoking history for evaluation of acute chest pain. In the available view of the sinus rhythm, we see normal variant STE which probably meets STEMI criteria in V4 and V5. Triage ECG: What do you think?
They wanted to know if I would like them to activate the outside hospital's "STEMI alert." But of course, this is not a STEMI by definition as it does not meet STEMI criteria. The STEMI guidelines do state that hyperacute T-waves "may indicate early acute myocardial infarction" but do not discuss it as a "STEMI equivalent."
It was present on arrival at triage but then resolved before bed placement in the ED. Patient still not having chest pain however this is more concerning for OMI/STEMI. Wellens' syndrome is a syndrome of Transient OMI (old terminology would be transient STEMI). It is a ssociated with mild dyspnea on exertion. Aspirin given.
It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. No appreciable skin pallor. He denied any known medical history, specifically: coronary artery disease, hypertension, dyslipidemia, diabetes, heart failure, myocardial infarction, or any prior PCI/stent. Is this OMI?
EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I said "Not OMI.
This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. Below is the initial ED ECG. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI. Does this suggest a change in location of escape mechanism, specifically from Junctional to Ventricular?
He had walked into the ED (did not use EMS). Thus, this is both an anterior and inferior STEMI. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. Exact pain history was difficult to ascertain. There was some SOB. Could it be acute (vs.
You can subscribe for news and early access (via participating in our studies) to the Queen of Hearts here: [link] queen-form This EMS ECG was transmitted to the nearby Emergency Department where it was remotely reviewed by a physician, who interpreted it as normal, or at least without any features of ischemia or STEMI.
This certainly looks like an anterior STEMI (proximal LAD occlusion), with STE and hyperacute T-waves (HATW) in V2-V6 and I and aVL. On arrival to the ED, this ECG was recorded: What do you think? How do you explain the anterior STEMI(+)OMI immediately after ROSC evolving into posterior OMI 30 minutes later?
[link] Case continued She arrived in the ED and here is the first ED ECG. STEMI MINOCA versus NSTEMI MINOCA STEMI occurs in the presence of transmural ischaemia due to transient or persistent complete occlusion of the infarct-related coronary artery. I don't know if her pain was getting better or not. From Gue at al.
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. The patient was transported to the ED. Here is his ED ECG: There is sinus tachycardia. Is this acute STEMI? Is this an acute STEMI? -- Unlikely!
Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case. Thus, this is obvious STEMI(+) OMI until proven otherwise.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content