This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
We will be using redacted information from different cases where paramedics attempted TCP in the field. In this call, paramedics arrived on scene to find a patient apneic and pulseless with CPR in progress by first responders (AED had an unknown unshockable rhythm). The paramedics initially set the current at 60mA.
We will be using redacted information from different cases where paramedics attempted TCP in the field. The paramedics begin CPR. Two paramedics are in the rear of the ambulance managing resuscitation (another crew had arrived and provided support with a driver). On ED arrival ROSC is achieved.
As an EM physician, he shares how he decides to care for his own patients in the ED who present with rapid atrial fibrillation. He wants paramedics to ask the same question he asks: Is the rapid A-fib the primary problem or secondary to another critical condition like sepsis, PE, DKA, hypovolemia, etc?
Date: February 28, 2024 Guest Skeptic: Dr. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Case: A 59-year-old man walks into your community emergency department (ED) complaining of chest pain.
Before attending medical school, he was a New York City Paramedic. He currently practices emergency medicine in New Mexico in the ED, in the field with EMS and with the UNM Lifeguard Air Emergency Services. Case: You are working as a paramedic, and you respond to a cardiac arrest.
Date: April 25, 2024 Guest Skeptic: Missy Carter is a PA working in an ICU in the Tacoma area and an adjunct faculty member with the Tacoma Community College paramedic program. When emergency department (ED) staff roll her to remove her clothing her humeral intraosseous (IO) is dislodged. February 2024.
In this episode, we discuss a recent paper on false electrical capture and pre-hospital transcutaneous pacing by paramedics. The guests, Tom Boutilet, Josh Kimbrell, and Judah Kreinbrook, discuss their research findings and the implications for paramedics. Prehosp Emerg Care. 2024 Mar 15:1-9. doi: 10.1080/10903127.2024.2321287.
The patient is not responsive and the paramedics cannot get a blood pressure. So I did what we as ED physicians are all so good at – I prepared. I meet the paramedics at the door. We had sent off a Type and Screen as soon as the patient arrived at the ED. We have a knife stab wound to the chest or abdomen coming.
However, RSI has never been shown to reduce the risk of aspiration in the ED (13) or during emergent OR cases (14). While RSI should remain the gold standard in the vast majority of patients in the ED, FI presents an additional technique to mitigate anatomic or physiologic risk. To date, ketamine has been the agent of choice (12).
The majority of our students come from a premedical background but there are a few with other career choices such as firefighter, paramedic, law enforcement, etc. You get the benefit of working with a paramedic without going to medic school. This is a position that is also sought after by nursing assistants as well as paramedics.
Background : Emergency Department (ED) overcrowding limits patient care in the prehospital and hospital system. A program was implemented to decrease the time to patient handoff from EMS arrival to ED staff, also known as the delivery interval and total turnaround interval.
At one of the hospitals, while my partner finished up the run form in the passenger seat –shed teched the call–I announced I was going back into the ED to the EMS room to see if they had any pizza. When I focused on her, she asked if I liked being a paramedic. I love being a paramedic for a lot of reasons.
Priorities are changing in prehospital care, with many paramedics now questioning career commitment for the future. National industry insight reporting from the Australian Industry and Skills Committee suggests that, in 2019 alone, Australia wide, there were over 4,500 enrolments in ambulance and paramedic qualifications1.
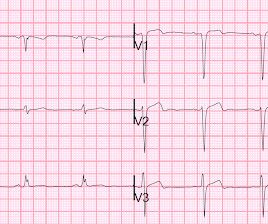
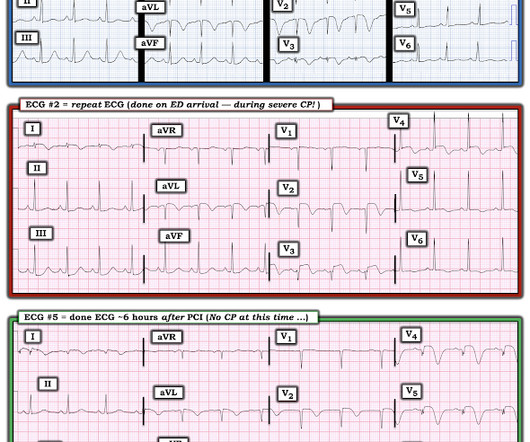
The first (and only) ED ECG is here: QTc 386. A prospective analysis of consecutive adult patients presenting to an urban/suburban two paramedic ambulance service fromJuly 15, 2006, to August 15, 2007, who have diagnostic ECGs for STEMI. A second ECG was done prior to arrival at the ED. Most ST elevation is resolved.
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. The young ED tech immediately suspected LAD OMI.
One barrier to including children in such programs is a lack of evidence regarding whether paramedics and emergency medical technicians (EMTs) can accurately identify children with low-acuity complaints. Our primary objective was to compare the accuracy of EMTs to that of paramedics in identifying low-acuity pediatric encounters.
JAMA May 2018 Guest Skeptic: Missy Carter, former City of Bremerton Firefighter/Paramedic, currently a physician assistant practicing in emergency medicine in the […] The post SGEM#271: Bougie Wonderland for First Pass Success first appeared on The Skeptics Guide to Emergency Medicine. Bougie use may be helpful in ED intubation.”
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC?
A 32 year old male presents to ED after cutting his right cubital fossa in a suicide attempt. According to the paramedics there was a large amount of blood on scene.
A 32 year old male presents to ED after cutting his right cubital fossa in a suicide attempt. According to the paramedics there was a large amount of blood on scene.
A 65 year old female is brought to ED via ambulance on a priority 1. According to the paramedics the patient has taken an overdose of benzodiazepines and alcohol. Her GCS is 3 and the team is prepa…
A 65 year old female is brought to ED via ambulance on a priority 1. According to the paramedics the patient has taken an overdose of benzodiazepines and alcohol. Her GCS is 3 and the team is prepa…
A 65 year old female is brought to ED via ambulance on a priority 1. According to the paramedics the patient has taken an overdose of benzodiazepines and alcohol. Her GCS is 3 and the team is prepa…
A 65 year old female is brought to ED via ambulance on a priority 1. According to the paramedics the patient has taken an overdose of benzodiazepines and alcohol. Her GCS is 3 and the team is prepa…
Guest Skeptic: Clay Odell is a Paramedic/RN for New London Hospital EMS in New Hampshire, USA which provides 9-1-1 coverage and Mobile Integrated Healthcare […] The post SGEM#269: Pre-Hospital Nitroglycerin for Acute Stroke Patients? The Lancet March 2019. The Lancet March 2019. He has a history of hypertension.
Circulation 2020 Guest Skeptic: Missy Carter is a PA practicing in emergency medicine in the Seattle area and an adjunct faculty member with the Tacoma Community College paramedic program. Survival After Intravenous Versus Intraosseous Amiodarone, Lidocaine, or Placebo in Out-of-Hospital Shock-Refractory Cardiac Arrest.
In-home nurse practitioner visits, same day specialist appointments and Community Paramedic check-ins represent examples of services that VBCOs can offer to better serve patients whose circumstances may not indicate admission but demonstrate a need for a higher level of care.
He is also now a fully fledged “sonologist” Casey currently splits his time between Broome, a small rural hospital in the remote Kimberley region of Western Australia, and a large tertiary ED in sunny Perth. They have two large bore intravenous (IV) access and are planning to bring them to your ED as soon as possible.
Below is the first ECG recorded by paramedics after 2 hours of chest pain, interpreted by the machine as “possible inferior ischemia”. In isolation this ECG does not show OMI, but following the paramedic ECGs this indicates spontaneous LAD reperfusion. It’s unclear if the paramedic ECGs were seen or missed in the ED.
He is interested and experienced in healthcare informatics, previously worked with ED-directed EMR design, and is involved in the New York City Health and Hospitals Healthcare Administration Scholars Program (HASP). The paramedics achieve return of spontaneous circulation (ROSC) after CPR, advanced cardiac life support (ALCS), and Intubation.
We know instinctively that the years of running calls, driving incessantly, long hours posted, and inherent risks of being a paramedic or EMT will get us back in the end. Reflecting on my career and practice; and as I struggle with my place on the burnout continuum, I tried to remember the times when I like being a paramedic the most.
Ed Bauter We’ve all been there. The design of the study allowed the paramedics to use discretion when placing an airway in the patients that were introduced to the study. It certainly is not representative of paramedic on the whole. What’s the right airway to use? On paper, this is an easy thing to do.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (Ret) @DidlakeDW Expert contribution by Dr Robert Herman @RobertHermanMD @PowerfulMedical (Chief Medical Officer) An adult male called 911 for new-onset epigastric burning. To which the lead paramedic replied, “Not cardiac; his symptoms are atypical. Is this OMI?
David Didlake, FF/EMT-P, AG-ACNP @DidlakeDW An elder female presented to the ED with worsening shortness of breath. Pharmacology Review Digoxin is probably one of those medications vaguely recalled from paramedic school. She was known to have a history of poorly controlled COPD, AFib, and multivessel coronary disease.
Madden, Paramedic. An interesting comment provided by Paramedic Madden is that a few team members initially interpreted the T wave presentation as hyperkalemia, as opposed to occlusive hyperacuity. Let's revisit the deWinter occlusion provided by Paramedic Madden. Chou's Electrocardiography in Clinical Practice, 6th ed.
Due to this, it’s important for the industry to develop strategies for better supporting psychiatric patients while avoiding unnecessary ED visits and secondary EMS transports. For Eagle County Paramedic Services, turning to MIH was integral to helping them provide services for their underserved population while also saving millions in costs.
David Didlake Firefighter / Paramedic Acute Care Nurse Practitioner @DidlakeDW Peer review provided by Dr. Steve Smith [link] @SmithECGBlog An adult female called 911 for chest discomfort and difficulty breathing. The following ECG was captured upon arrival at the receiving ED. The ED resulted an 8.7 The serum K returned 8.7,
The tachycardia was gone by the time paramedics arrived. First ED ECG is Wellens' (pain free). First responders found him to be very tachycardic , confused, perserverating and with no memory of the event. There was tongue biting. Lightheadedness continued. He had a prehospital ECG: What do you think? Interpretation.
Sinha 2012] It is useful in the prehospital setting , correlating well with actual weight and ED Broselow weight. Accuracy of paramedic Broselow tape use in the prehospital setting. Good correlation to bed scale weight in trauma patients (Pearson coefficient 0.86), but there was some error in the highest weight category.
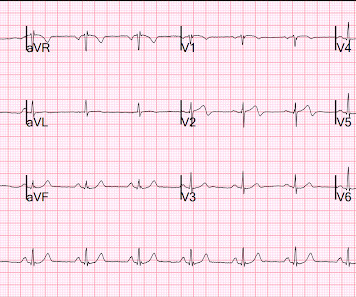
An ED ECG, if recorded with pain, should show LAD OMI. Smith — in the setting of a patient with new chest pain — the initial ECG in today's case ( = ECG #1 — obtained by the EMS team prior to ED arrival ) — is diagnostic of ACS ( A cute C oronary S yndrome ) until proven otherwise.
Prior to earning his MD, he worked as a paramedic in the New York City 911 system. Case: A 43-year-old male presents to your emergency department (ED) the day after being involved in an all-terrain vehicle (ATV) accident. He is also a resident flight physician with UNM’s aeromedical service, UNM Lifeguard.
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic @DidlakeDW A 50 y/o Male was taking his dog for a leisurely stroll through the park when he suddenly experienced new onset chest discomfort. He waited for it to subside, but after 30 minutes of persistence he called 911. However, when the Troponin I returned 8.4
The PREOXI trial compared oxygen mask pre-oxygenation versus noninvasive positive-pressure ventilation (NIPPV) in patients requiring intubation in emergency departments (EDs) and intensive care units. 2 This was not an ED trial but was performed in stable patients on the inpatient wards. The obvious winner was NIPPV, whose 9.1
David Didlake Acute Care Nurse Practitioner Firefighter / Paramedic (ret) @DidlakeDW Expert commentary and peer review by Dr. Steve Smith [link] @smithECGBlog A 57 y/o Female with PMHx HTN, HLD, DM, and current use of tobacco products, presented to the ED with chest discomfort. A 12 Lead ECG was captured on her arrival.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content