This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Let’s consider Inborn Errors of Metabolism Presenting in the ED : Inborn Errors of Metabolism: Basics Common Presentations, Uncommon Kiddos For the child with lethargy, vomiting, acidosis, hypoglycemia , organomegaly, or cardiopulmonary arrest remember to consider Inborn Errors of Metabolism (IEM) on your DDx. Samantha A.
Hosts: Joe Offenbacher, MD Audrey Bree Tse, MD [link] Download Leave a Comment Tags: Anticoagulation , Critical Care , Resuscitation Show Notes Coagulation Cascade: Algorithm for Anticoagulated Bleeding Patient in the ED: Indications for Anticoagulation Reversal: References: Baugh CW, Levine M, Cornutt D, et al. Iran J Pharm Res.
It’s a busy day in the paediatric ED. The osmolar gap measures the difference between the measured plasma osmolality and the calculated plasma osmolality , providing an estimate of unmeasured solutes in the blood. Glucose] is the plasma glucose concentration (mg/dL). Back to our toddler in the ED.
It is commonly missed during the first few ED visits. First line therapies for anti-NMBDA receptor encephalitis consists of… High dose steroids , IVIG, and PLEX – Therapeutic plasma exchange Only 50% of patient’s respond, and will require second line therapies such as Rituximab. Moral of the Morsel It’s NOT always psych!
sodium chloride), and balanced crystalloid solutions, meaning those with a chloride composition closer to plasma such as lactated ringer’s or Plasma Lyte 148. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates.
He is also now a fully fledged “sonologist” Casey currently splits his time between Broome, a small rural hospital in the remote Kimberley region of Western Australia, and a large tertiary ED in sunny Perth. They have two large bore intravenous (IV) access and are planning to bring them to your ED as soon as possible.
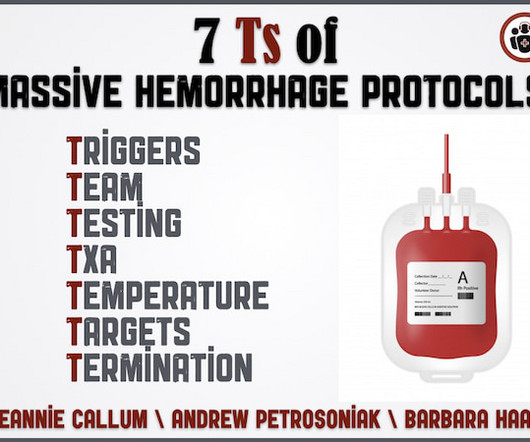
Why is serum calcium important to draw in the ED for the patient who is exsanguinating? If someone is on anti-platelets or anticoagulants what is the best strategy to ensure the docs in the ED know what to give and how much? What should be the lab resuscitation targets? How do we mitigate the risk of hypothermia? When and how much TXA?
Now, let’s discuss another complication of “The Great Mimicker” which may throw us for a loop in the ED – Pseudoparalysis of Parrot : Pseudoparalysis of Parrot – Basics First described by Jules Marie Parrot in 1871. We have touched on the treatment for older children with syphilis with Bicillin CR vs LA.
Note that succinylcholine is contraindicated as it is metabolized by plasma pseudocholinesterase. Use benzodiazepines such as diazepam or midazolam for seizures. Provide supportive care. The patient will likely require intubation. Even with rapid treatment, the mortality rate is high. Vikhyat Bebarta, Bryan Judge, and Louise Kao. McGraw Hill.
Bradykinin Mediated Plasma globulins called kininogens release bradykinin and cause vascular permeability. Image: ( Morgan 2010 ) Features Absence of urticaria and pruritus Insidious onset (24-36 hours) ACE Inhibitors Inhibition of ACE hinders the degradation of bradykinin and can lead to idiosyncratic angioedema.
Case: A 71-year-old man is brought to your emergency department (ED) by emergency medical serviced (EMS) having fallen two steps at home. The transfusion tech calls to remind you that your protocol is currently under review, and asks if would you like the 1:1 or the 1:3 version of fresh-frozen plasma (FFP) to packed red blood cells (pRBC)?
Some bench work, observational studies, and now two large, unblinded, cluster-randomized single-center trials ( SMART and SALT-ED ) suggested a benefit to using balanced crystalloids (i.e. The SALT-ED trial was also a single-centre unblinded trial, but the primary outcome was hospital free days. Reference: Zampieri et al.
It's important to keep in mind that you are not functioning as an EMT when you're an ED Tech/Assistant. You’ll be working closely with providers of various levels while seeing a variety of medical illnesses and traumatic injuries depending on the hospital you work at.
Background Around 6 million people in the U.S. 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. Background Around 6 million people in the U.S.
These medications are a vital tool in the care of ED patients, from simple local analgesia for a laceration repair to regional analgesia for painful procedures. Metabolism of ester anesthetics is by plasma cholinesterase, whereas amides are metabolized by the cytochrome P450 system in the liver. [6] lidocaine) or an ester (e.g.,
JAMA 2015 [7] The PROPPR Trial 680 severely injured adult trauma patients Patients randomized to Plasma, Platelets, and PRBCs in a 1:1:1 ratio vs 1:1:2 ratio No difference in overall mortality at 24 hrs BUT 1:1:1 achieved hemostasis faster and fewer experienced death due to exsanguination at 24hrs Crombie N et al. Ann Emerg Med.
Congenital Syphilis may still occur in patients presenting to your ED! Can identify T. pallidum before antibodies against it can be detected. > 4 weeks of age : Aqueous crystalline penicillin G 50,000 Units/kg IV every 6 hours Treat for 10-14 days. Causes fevers , hypotension , and can be life-threatening.
All you know, back in ED, is that the ETA is 10 minutes, and there is a single stab wound to the chest. The ODP is caught up leaving theatres and has not yet made it down to ED. The trauma call goes out. You will be running the show today, and you want to use your preparation time well. to −0.5%]; P = 0.03.). to −0.5%]; P = 0.03.).
3 Measured in analytical testing : Laboratories measure plasma concentration using osmometers which measures values as a function of kilograms of solvent. Choice of the best equation for plasma osmolality calculation: Comparison of fourteen formulae. Validation of equations used to predict plasma osmolality in a healthy adult cohort.
Most of the hyponatraemia we see admitted through the ED will be hypoosmotic hyponatraemia. This time the tonicity is high from something else such as high glucose or mannitol drawing water from cells into plasma. Most of the hyponatraemia we see admitted through the ED will be hypoosmotic hyponatraemia.
Older person presents to the ED after being unwell for several weeks. If it’s rising too quick it’s often because the patient is losing lots of water through the kidneys which concentrates the plasma raising the Na in the blood. Older person presents to the ED after being unwell for several weeks.
Two randomized controlled trials by Moore et al found that prehospital plasma administration in trauma patients is associated with hypoCa (53% vs 36%). How does this impact what you do in the ED? How does this impact the prehospital environment? Prehospital blood product transfusion increases risk of hypoCa.
A 37-year-old G2P2 female with no other past medical history presents to the ED with a 2-day history of intermittent fever and foul-smelling vaginal discharge. Plasma cell endometritis is associated with Chlamydia trachomatis infection. We’ll keep it short, while you keep that EM brain sharp. What is the diagnosis? PMID: 9067792.
DEG is rapidly absorbed when ingested and can reach peak plasma and brain tissue concentrations within four hours of ingestion. “Diethylene Glycol” in Goldfrank’s Toxicologic Emergencies , 11e Eds. “Fomepizole” in Goldfrank’s Toxicologic Emergencies , 11e Eds. Schier, Capt. Nelson, et al.
2,3 Here we examine some of the evidence behind the various components of MTPs, specifically calcium and factor VIIa, and the ratios in which the main products of red blood cells, plasma, and platelets should be administered. What is the ideal blood component ratio for massive transfusion in traumatic hemorrhage? 248(3):447-58.
Case: A 45-year-old woman presents to the emergency department (ED) with itching to bilateral palms. 5 Identification of obstructive physiology in the emergency department (ED) and referral for definitive management can spare patients from these damaging downstream consequences. Her triage vitals are within normal limits.
Not so much for the patient but it’s one of those ones that is niche enough to not have been picked up via the usual filters of ED, medical team to the ward. Treatment consists of: * PLEX – actual proper PLEX with plasma replacement as opposed to just washing out all the good stuff and giving albumin as replacement.
2 TTP often presents abruptly, and most patients that develop it first visit the emergency department (ED) as their symptoms worsen. 1 Pregnant patients are particularly vulnerable to misdiagnosis of TTP in the ED. Most of these deaths can be attributed to a delay in diagnosis. Thus, early management is essential for patient outcomes.
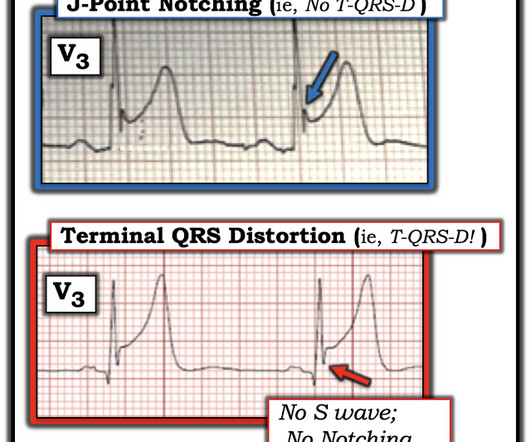
Here is his ED ECG: There is obvious infero-posterior STEMI. Internal potassium balance and the control of the plasma potassium concentration. Plasma potassium ([K] p ) was measured at 15-minute intervals during and after the infusion in 31 patients. Medics stated that he had not been taking his clopidogrel for 2 weeks.
Schnapp, MD, MEd (Associate Program Director, University of Wisconsin) // Reviewed by: Joshua Lowe, MD (EM Attending Physician, USAF), Marina Boushra (EM-CCM, Cleveland Clinic Foundation); Brit Long, MD (@long_brit) Case A 36-year-old pregnant woman at 21 weeks gestation presents to the ED with chest pain.
Terbutaline and Albuterol for Lowering of Plasma Postassium Initial labs returned and confirmed critical hyperkalemia and new renal failure. He ended up requiring a total of 13 grams of CaCl in the ED to maintain rhythm and hemodynamics until our dialysis colleagues could start dialysis in the ED.
They transported to the ED. The history, obtained subsequently, is interesting: The patient had been seen at an outside ED 2 days prior and the K was 2.5 Hospital admission had been recommended, but she left that ED against medical advice. Internal potassium balance and the control of the plasma potassium concentration.
Moreover, LTOWB also allows us to administer platelets and plasma, in addition to red cells, to promote clotting and homeostasis. If you don't have access to LTOWB and are administering component therapies such as PRBCs or plasma, this is still incredible and I highly encourage it! Linden JV, Bianco C, eds. Transfusion.
An 18-year-old woman presented to the emergency department (ED) with symptoms of nausea, vomiting, diarrhea, and abdominal pain. Before arriving at our ED, the patient sought care at an urgent care clinic, where she was prescribed ondansetron without improvement. Jamaican vomiting sickness in Toledo, Ohio. Ann Emerg Med.
On arrival to the ED, the patient was diaphoretic, tachycardic. I did not think it was due to ACS, but we ordered an ED ECG immediately: What do you think? Peak plasma concentration of amphetamines is rapid ( within minutes ) following inhalation or injection. and had dilated pupils. He was alert and oriented.
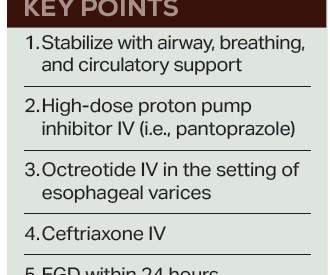
Fresh frozen plasma, or FFP, should only be given to cirrhotic patients as part of the massive transfusion protocol in cases of profound hypotension, as “patients with cirrhosis rarely have true enzymatic hypocoagulability, and FFP may worsen bleeding due to over-resuscitation and dilution of coagulation factors.” 6 Balloon tamponade (i.e.,
In fact, there is laboratory evidence that CO toxicity increases Plateletneutrophil aggregates and plasma myeloperoxidase (MPO) concentration and thus may precipitate ACS (though this is by no means clinically proven). Figure-1: Comparison of the initial ECG in the ED ( = ECG #1 ) with the follow-up ECG done the next day ( = ECG #2 ).
This response varies between individuals, age groups and developmental stages, so a single plasma concentration cannot be defined. How do I measure hypoglycaemia in the ED? If there is clinical concern for hypoglycaemia, plasma glucose concentration should be measured. Plasma glucose Beta-hydroxybutyrate (i.e.
The nuances of fracture patterns and delineating mechanically unstable pelvic fractures from stable ones is less important to the ED. This is less critical in ED management of the unstable pelvic fracture, as the optimal site for identification of rectal or vaginal tears is the operating room.
On arrival to the ED, her blood pressure is 84/36 mmHg with a heart rate of 110 beats per minute. 3,4 Prompt recognition and management of sepsis and septic shock are paramount for the ED clinician. 8,9 Recently, monocyte distribution width (MDW) has shown promise in a large meta-analysis as a useful screening tool in the ED.
F, HR 48, RR 28, BP 104/62, SPO2 88% on non-rebreather mask The patient’s friend who brought her to the ED tells you the patient made suicidal statements earlier in the day and was found in her yard shed. These are send-out labs with turn-around times that make them unlikely to affect the ED course or guide treatment. CorePendium.
These are send-out labs with turn-around times that make them unlikely to affect the ED course. This prevents ongoing exposure to the patient and ED staff. In: Mattu A and Swadron S, ed. 3 However, may be helpful in diagnosing the chronic toxicity forms. Iran Red Crescent Med J 16: e5072, 2014. Pesticides and Cholinergics.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content