This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Date: February 28, 2024 Guest Skeptic: Dr. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Case: A 59-year-old man walks into your community emergencydepartment (ED) complaining of chest pain.
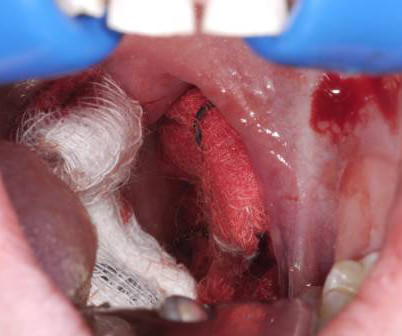
A young woman, 13 days post-tonsillectomy, comes into your rural emergencydepartment (ED) coughing up blood. The literature suggests that approximately 85 percent of these cases require procedural source control in the operatingroom, highlighting the importance of expediting transport arrangements.
EmergeNcyDepartment use of Apneic Oxygenation versus usual care during rapid sequence intubation: A randomized controlled trial (The ENDAO Trial). EmergeNcyDepartment use of Apneic Oxygenation versus usual care during rapid sequence intubation: A randomized controlled trial (The ENDAO Trial). Reference: Caputo et al.
Differences in intubation outcomes for pediatric patients between pediatric and general EmergencyDepartments. Intubation practice and outcomes among pediatric emergencydepartments: A report from National Emergency Airway Registry for Children (NEAR4KIDS). Acad Emerg Med. 0.41), p < 0.001.
Over the past few years, there has been an increase in emergencydepartment (ED) volumes and lengths of stay. The effect of emergencydepartment crowding on lung-protective ventilation utilization for critically ill patients. Paper: Owyang CG, et al. J Crit Care. N Engl J Med. 2000 May 4; PMID: 10793162 Harvey CE, et al.
PECARN prediction rule for cervical spine imaging of children presenting to the emergencydepartment with blunt trauma: a multicentre prospective observational study. Children in the validation cohort were admitted to the intensive care unit or operatingroom less frequently than those in the derivation cohort.
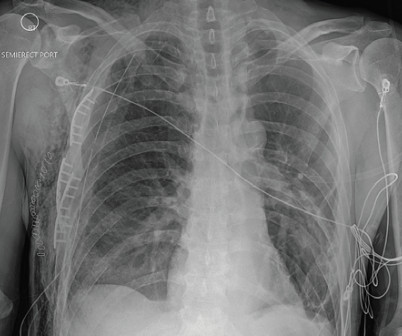
A 58-year-old male with a history of alcohol abuse presented to the emergencydepartment (ED) as a category 2 trauma for a fall with a reported flail chest. EMS recognized a chest wall deformity with movement of the chest wall, and a splint was devised and taped around his chest for what was suspected to be a flail chest.
If pre-made syringes are not financially feasible then the creation of these medications should be done by a dedicated emergencydepartment pharmacist. Clinical Bottom Line: Acute hypotension must be treated emergently in order to decrease morbidity and mortality. Am J Emerg Med. J Med Toxicol. Epub 2019 Jul 3.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. Per EMS, the patient was found at the bottom of a high voltage line with diffuse burns and amputation of his left forearm.
We’ll keep it short, while you keep that EM brain sharp. Operative management is required in majority of cases. 9,23 Disposition: Dislocation : If successfully reduced in the emergencydepartment may discharge with strict mobility restrictions and Orthopedic follow up. Initial vital signs include T 36.8, Hospitals, 2018.
C, respiratory rate 20 breaths per minute, and oxygen saturation 95% on room air. What is the EM physician’s role in the stabilization of unstable pelvic injuries? If a pelvic binder was placed by EMS, inquire whether this was placed empirically or if mechanical pelvic instability was already elicited.
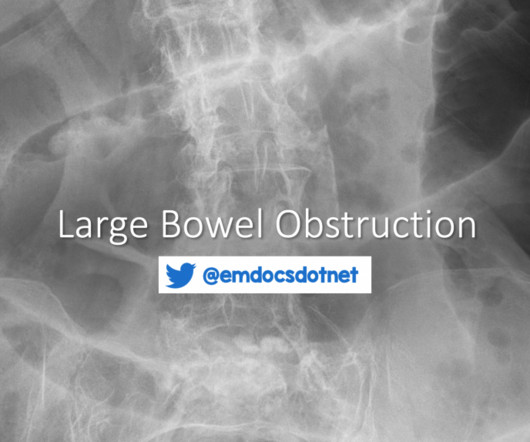
In these cases, CT may not be feasible and a plain radiograph showing free air or bedside US showing free fluid may be useful to confirm serious abdominal pathology prior to transfer to the operatingroom. He describes the pain as a gradually worsening pressure-like discomfort distributed across his entire abdomen.
Included patients from out-of-hospital, emergencydepartment, intensive care unit, and operating-room intubations. Intubation performed in all settings (out-of-hospital, emergencydepartment, ICU, and operatingroom). to 1.36). to 2.39) might outweigh the benefits. N Engl J Med.
The “syringe” technique: a hands-free approach for the reduction of acute nontraumatictemporomandibulardislocations in the emergencydepartment. J Emerg Med. Rosens Emergency Medicine: Concepts and Clinical Practice, 7 ed. Louis, Mosby, Inc., 2010, (Ch) 70: p 895-909. GorchynskiJ et al. 2014; 47(6):676-81.
Earlier in the summer, I wrote a blog discussing the challenges, intricacies, and educational pitfalls of postpartum hemorrhage in EMS. For patients suffering from intrapartum cardiac arrest, I would encourage you to transport the patient as expeditiously, but safely, as possible to the closest emergencydepartment.
An EM Residents Guide to Basic Airway Management Authors: Justin Rice, MD Sagar Desai, MD Eunice Monge, MD William Chiang, MD Preface: Airway management is one of the most critical skills in emergency medicine, yet it can be one of the most challenging to master. Ann Emerg Med. ” Academic Emergency Medicine 26.9
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content