This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
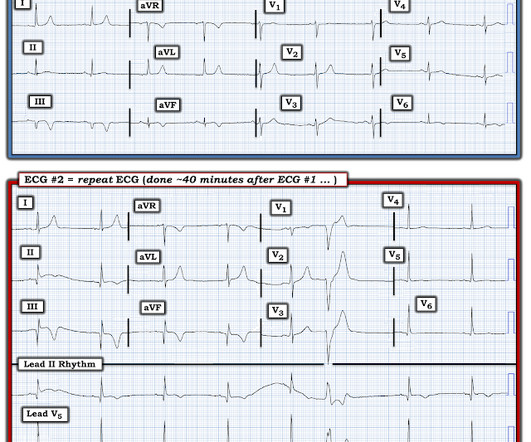
Major adverse cardiac events 40 minutes after giving the antiarrhythmic. The following table shows their results, take a look: Note that procainamide leads with less adverse cardiac events. Procainamide therapy was associated with less major cardiac adverse events and a higher proportion of tachycardia termination within 40 min.
, tells us that we physicians do not need to even look at this ECG until the patient is placed in a room because the computer says it is normal: Validity of Computer-interpreted “Normal” and “Otherwise Normal” ECG in EmergencyDepartment Triage Patients I reviewed this article for a different journal and recommended rejection and it was rejected.
The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. Diagnosis of Type I vs. Type II Myocardial Infarction in EmergencyDepartment patients with Ischemic Symptoms (abstract 102). Murakami MM.
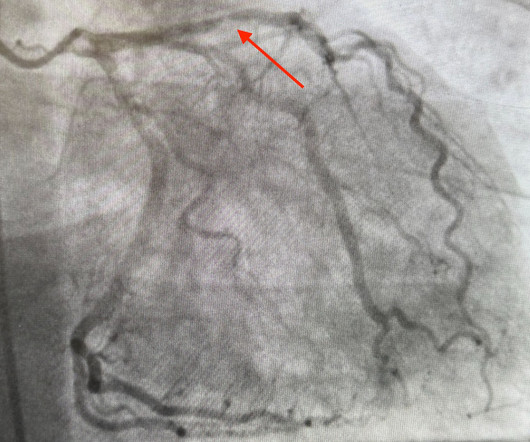
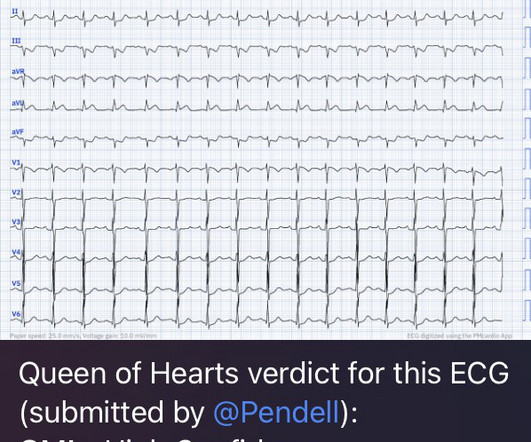
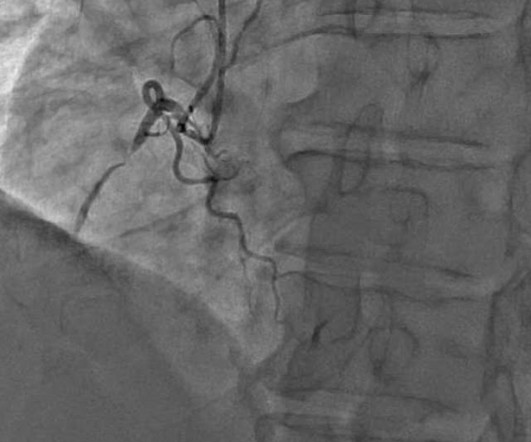
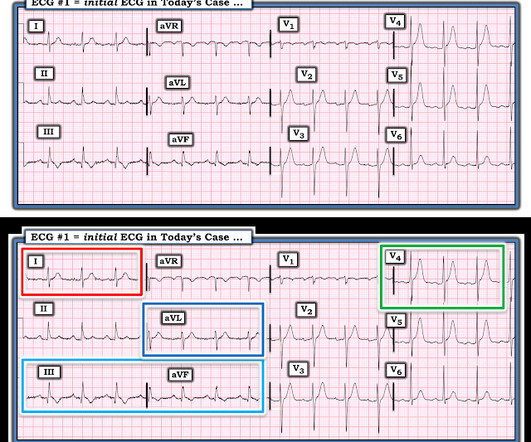
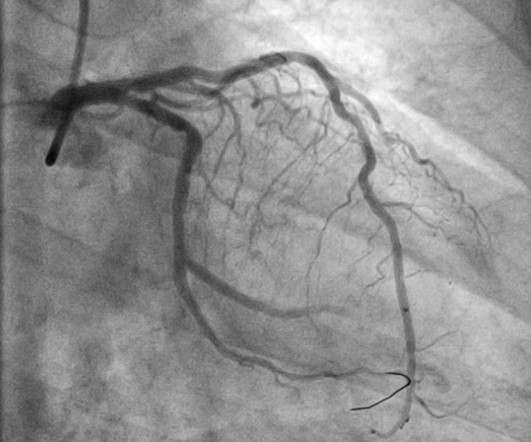
Quiz : What percent of full blown STEMI have an open artery with normal flow at angiogram? It too is "normal" and you decide that this is not OMI or STEMI and you just decide to get troponins. So despite the artifact — and even without any history — this initial ECG has to be interpreted as an acute event until proven otherwise.
Upon arrival to the emergencydepartment, a senior emergency physician looked at the ECG and said "Nothing too exciting." Takotsubo is a sudden event, not one with crescendo angina. Even in patients whose moderate stenosis undergoes thrombosis, most angiograms show greater than 50% stenosis after the event.
This was sent by anonymous The patient is a 55-year-old male who presented to the emergencydepartment after approximately 3 to 4 days of intermittent central boring chest pain initially responsive to nitroglycerin, but is now more constant and not responsive to nitroglycerin. It is unknown when this pain recurred and became constant.
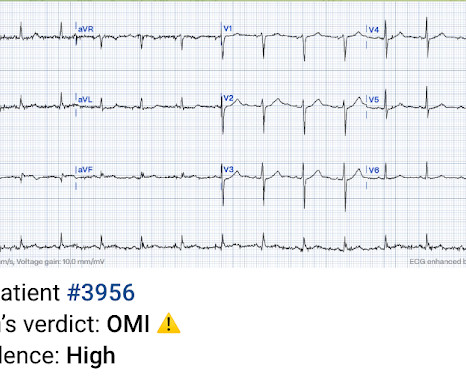
QOH versions 1 and 2 both say Not OMI, with high confidence, without any clinical context, despite the abnormal STE meeting STEMI criteria. Context: a man in his 40s presented to the emergencydepartment with 1 day of sudden onset chest pain. I sent this to our group without information and Dr. Smith responded: "Not OMI.
STEMI , ST-segment elevation acute myocardial infarction ). 1 Initial diagnosis of STEMI ECG Management Recommendation Level of evidence A 12-lead ECG should be interpreted immediately (within 10 minutes) at first medical contact. I B Designated PCI centres should provide angiography and reperfusion 24/7 without delay.
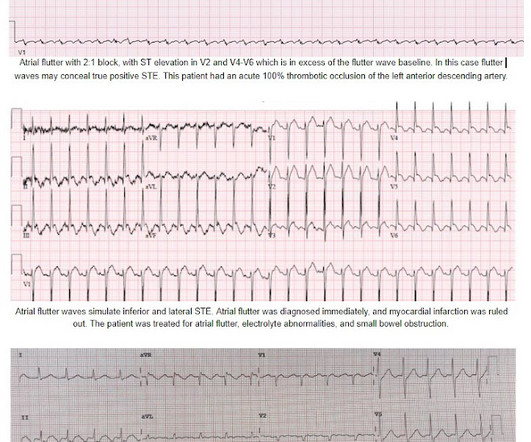
A 56 year old male with a history of diabetes, dyslipidemia, hypertension, and coronary artery disease presented to the emergencydepartment with sudden onset weakness, fatigue, lethargy, and confusion. At 2111, the troponin I peaked at 12.252 ng/mL (this is in the range of STEMI patients, quite high).
Is this inferor STEMI? Atrial Flutter with Inferior STEMI? Inferolateral ST elevation, vomiting, and elevated troponin The treating team did not identify the flutter waves and they became worried about possible "STEMI" (despite the unusual clinical scenario). The EM provider asked if the cardiologist thought it was a "STEMI."
A 35-year-old male presented to the emergencydepartment complaining of chest pain that started 1.5 5 Studies looking at this phenomenon in the emergencydepartment setting for patients presenting with chest pain are lacking. Dr. Young is an emergency physician at Saint Francis Hospital and Medical Center, Hartford, Conn.
It was ongoing on arrival in the emergencydepartment. But because there was no new ST elevation, the ECG was signed off as “STEMI negative” and the patient waited to be seen. The emergency physician was called to see the patient 90 minutes later after the troponin I returned at 1100 ng/L. What do you think? Take home 1.
A man in his 60s with a history of severe alcohol use disorder and epidural abscess on long-term ciprofloxacin presented to the emergencydepartment after an episode of syncope while standing in line at a grocery store. Is it STEMI? Written by Sean Trostel MD, peer reviewed by Meyers, Smith, Grauer, etc. What is going on here?
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the EmergencyDepartment with severe intermittent chest pain. Barely any STE, and thus not meeting STEMI criteria. Only now that the patient has STEMI criteria is he allowed to go to the cath lab, at around 0530.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Am J Emerg Med 2020 3. Backus BE, Six AJ, Kelder JC, et al. As per Drs.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergencydepartment with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. New ST elevation diagnostic of STEMI [equation value = 25.3
The remainder of his EmergencyDepartment stay was uneventful. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." He had no symptoms of ACS.
I finished my residency of Emergency Medicine and I’m working at a great EmergencyDepartment here in Brazil. Since then, I started looking for OMI EKG findings and not just STEMI. mm in lead I, thus not STEMI criteria) and was finally understood by the cardiologist.
While in the emergencydepartment, he undergoes an additional ECG: 00:49 - Not much change Second ECG with measurements and calculations Magnified view of second ECGs measurements and calculation It is still "negative" for LAD occlusion (less than 23.4) Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
[link] Angiography after Out-of-Hospital Cardiac Arrest without ST-Segment Elevation An RCT showing no advantage to routine immediate angiography in non-STEMI OHCA. link] Invasive Bacterial Infections in Afebrile Infants Diagnosed With Acute Otitis Media Afebrile infants ≤ 90 days diagnosed with AOM do not seem to be at risk for IBI.
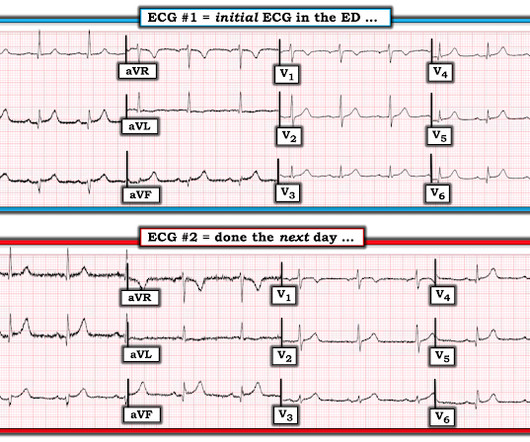
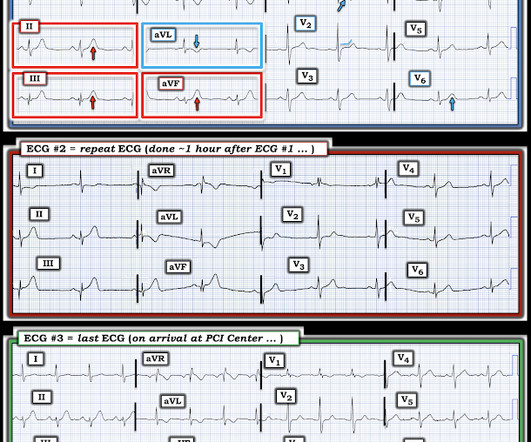
She was brought to the EmergencyDepartment and this ECG was recorded while she was still feeling nauseous but denied chest pain, shortness of breath, or other symptoms: What do you think? This one likely does meet STEMI criteria in II, III, and aVF. Criteria for a STEMI are definitely not met in ECG #1. What happened?
Submitted and written by Megan Lieb, DO with edits by Bracey, Smith, Meyers, and Grauer A 50-ish year old man with ICD presented to the emergencydepartment with substernal chest pain for 3 hours prior to arrival. The most recent event had occurred just before being triaged. Triage EKG: What do you think?
Clin Chem [Internet] 2020;Available from: [link] Smith mini-review: Troponin in EmergencyDepartment COVID patients Cardiac Troponin (cTn) is a nonspecific marker of myocardial injury. 12 All STEMI patients had very high cTn typical of STEMI (cTnT > 1.0
The patient’s ECG on arrival at the emergencydepartment is shown below. Add in the fact that symptoms began at least 24 hours ago — and these subtle-but-real ECG findings suggest a recent event until we can prove otherwise. He was expected to arrive at the tertiary care center within 60 minutes of the call.
A Deep Neural Network learning algorithm outperforms a conventional algorithm for emergencydepartment electrocardiogram interpretation. But lead V2 has a worrisome amount of ST elevation, and in a chest pain patient, I would be worried about STEMI. I do research on Cardiologs' algorithm: Smith SW et al. What an honor.
STEMI negative : the EMS automated interpretation read, “STEMI negative. According to the STEMI paradigm, the patient doesn’t have an acute coronary occlusion and doesn't need emergent reperfusion, so the paramedics can bring them to the ED for assessment, without involving cardiologists. Sinus bradycardia.”
There is worrisome T-wave inversion in inferior leads as well, which is another clue to LAD Occlusion In fact, this ECG meets STEMI criteria!! Why does the conventional algorithm not diagnose STEMI? Transient STEMI, serial ECGs prehospital to hospital, all troponins negative (less than 0.04
Case submitted and written by Dr. Mazen El-Baba and Dr. Emily Austin, with edits from Jesse McLaren A 50 year-old patient presented to the EmergencyDepartment with sudden onset chest pain that began 14-hours ago. This doesn’t meet STEMI criteria so in the current paradigm there’s no urgency to getting an angiogram.
There’s minimal concave ST elevation in III which does not meet STEMI criteria, so this ECG is "STEMI negative". Use STEMI criteria to identify acute coronary occlusion: the ECG was STEMI negative 2. A repeat ECG was done on way to cath lab: "STEMI negative" again. The cath lab was activated. Take home 1.
The is very small STE in III and aVF which do not meet STEMI criteria, hyperacute T waves, reciprocal TWI in aVL, and maximal STD in V2-V3 showing posterior OMI. The ECG was transmitted to the Emergency Medicine physician who recognized inferior and posterior OMI findings, and confirmed that the patient has potential ACS symptoms.
His first EKG is shown below, with a lead II rhythm strip: EKG 1, 1645 A provisder who is looking for STEMI would not see much in this EKG. It is possible that the T waves in this EKG are of an intermediate morphology between full-blown STEMI and inferior reperfusion. This is the classic morphology of hyperacute T waves.
1] In a review of hyperkalemia in the ED, all adverse events occurred prior to calcium and usually with multiple signs of hyperkalemia (like the first ECG) with the biggest predictors not only wide QRS, but also bradycardia and/or junctional rhythm.[2] Eur J Emerg Med 2020. West J Emerg Med 2017. References 1. Lindner et al.
A 69 year old woman with a history of hypertension presented to the emergencydepartment by EMS for evaluation of chest pain and shortness of breath. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI.
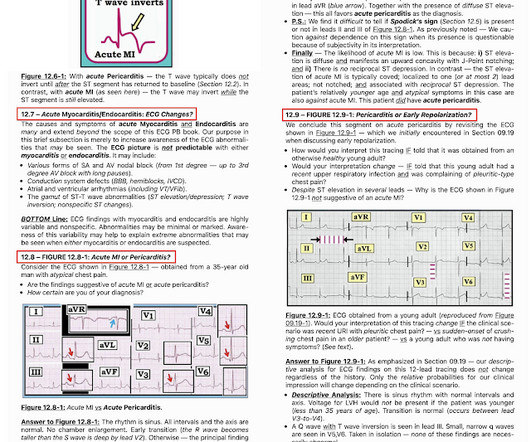
He presented to the emergencydepartment for evaluation. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). How extensive was this patient's heart disease prior to this recent event?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content