This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Do heroin overdose patients require observation after receiving naloxone? Guest Skeptic: Dr. Richard Hamilton (@RJHamiltonMD) is Chair of the Department of Emergency Medicine at Drexel University College of Medicine. Do heroin overdose patients require observation after receiving naloxone? Clinical Toxicology 2017.
He is also an avid FOAM supporter/producer through various online outlets including TheSGEM. […] The post SGEM#374: Bad Habits – Medications for Opioid Use Disorder in the EmergencyDepartment first appeared on The Skeptics Guide to Emergency Medicine. Date: August 23rd, 2022 Reference: Schoenfeld et al.
Hospital Observation Upon Reversal (HOUR) With Naloxone: A Prospective Clinical Prediction Rule Validation Study. Hospital Observation Upon Reversal (HOUR) With Naloxone: A Prospective Clinical Prediction Rule Validation Study. Sixty minutes after receiving naloxone he is GCS 15 and walking to the desk demanding to be discharged.
Naloxone will not reverse the effects of xylazine; however, it is routinely given in unresponsive or obtunded patients presenting with an opioid toxidrome. In patients with minimal response to naloxone, xylazine toxicity may be suspected [10]. Opioid overdoses involving xylazine in emergencydepartment patients: a multicenter study.
One study from a county in Massachusetts found that of all nonfatal opioid doses seen in the emergencydepartment from 2011-2015, 1 in 20 patients subsequently died within one year of initial visit with 66% of these deaths being directly related to an opioid overdose (4). PMID 33392580.
We do love to give out opiates in the emergencydepartment. However, does this trial apply to the emergencydepartment? Modified-release oxycodone-naloxone was the opiate of choice in this Australian trial. Kidney stone? Broken arm? Gunshot wound? Sore throat? Dexamethasone. And opiates. Spring into action, team!
Emergencydepartments (EDs) focus on rapid initiation of medical treatment. Patients with opiate overdose get naloxone. Once trust is established and patients are willing to accept calming medication, emergency physicians should consider these guiding principles. Patients with sepsis get antibiotics.
CASE A 30-year-old woman presents to the emergencydepartment with left arm pain from a chronic wound. While naloxone can treat fentanyl overdose, overdose symptoms may persist when xylazine is involved. Opioid overdoses involving xylazine in emergencydepartment patients: a multicenter study. Alexander RS, et al.
1 The emergencydepartment remains an important frontier for work in judicious prescribing, but opiate analgesia remains a valuable tool for the initial treatment of a variety of presentations. The addition of naloxone to the tablets may also provide a confounder in terms of the analgesia provided.
Bupe Allergy Buprenorphine induction has been the mainstay of emergencydepartment treatment of opioid use disorder for more than a decade [11, 12]. The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids.
A middle-aged male with squamous cell carcinoma and extensive metastases is brought to the emergencydepartment (ED) after being found unresponsive following a believed suicide attempt (SA) by methadone ingestion. Though paramedics administered naloxone, he remained somnolent. You order IV potassium and magnesium.
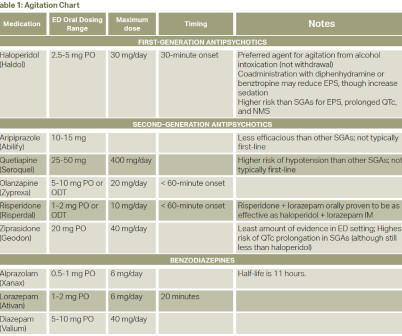
mg q20-30 min per dose) PRN naloxone in case of respiratory depression Some patients have SCD crises pain plan for reference Antimicrobials 11 Ceftriaxone + azithromycin if penicillin allergy for both children and adults. Left lower lung field end demonstrates expiratory wheezing on auscultation. Other lung fields unremarkable. C or 100.4
In the field, he was given 4 mg intranasal (IN) naloxone and rescue breaths via bag valve mask. He is administered 2mg intravenous (IV) naloxone and shortly after develops precipitated withdrawal with altered mental status, diaphoresis, vomiting, and diarrhea. When should a naloxone infusion be considered?
The pain worsened today, prompting him to come to the emergencydepartment for evaluation. Necrotizing fasciitis Case Question: Will naloxone reverse a xylazine overdose? The patient reported a wound to his left leg that had become larger over the past 5 months. BMP : Na 126; K+ 5.9; up from 0.69) ESR : >100 CRP : 15.94
This process of sickling and unsickling goes on and off until the erythrocyte membrane is no longer flexible. Irreversible sickle cells undergo either intravascular haemolysis or extravascular removal by the reticulo-endothelial system resulting in anaemia and splenic sequestration. Blood culture is pending. How would you evaluate this child’s pain?
A 33-year-old male with a history of drug use presented to the emergencydepartment (ED) for extreme agitation after receiving two doses of 2 mg naloxone by EMS for respiratory depression. It is illegal in six states and not regulated in 33 states. The pathophysiology of withdrawal from kratom use is not well studied.
There has been much speculation and the answer probably doesnt lie with one factor but with many, including increased availability of naloxone, the efforts of harm reduction workers, the end of the COVID isolation, the trend away from injecting to snorting or smoking, a less toxic drug supply, and expanded treatment.
Success at intubation likely takes more time and practice than other procedures, as shown in recent research on ED residents and their success rate at intubating, measured as a function of their total number of intubations (See Figure 1). Practice may not achieve perfection, but it will make you better. fiber optic through the nose).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content