This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A young woman, 13 days post-tonsillectomy, comes into your rural emergencydepartment (ED) coughing up blood. The literature suggests that approximately 85 percent of these cases require procedural source control in the operatingroom, highlighting the importance of expediting transport arrangements. CREDIT: Dr. P.
Differences in intubation outcomes for pediatric patients between pediatric and general EmergencyDepartments. Intubation practice and outcomes among pediatric emergencydepartments: A report from National Emergency Airway Registry for Children (NEAR4KIDS). Acad Emerg Med. 0.41), p < 0.001.
In 1901, UVA opened its first hospital with 25 beds and three operatingrooms. The emergencydepartment (ED) at UVA was rebuilt in 2019 and the department had not fully optimized its operations when COVID-19 hit. She is a consultant with Quality Matters Consulting, and her expertise is in ED operations.
In her spare time, Melissa also enjoys being the fellowship director to an amazing group of PEM trainees. Case: Brian is a 14-year-old male who presents to the emergencydepartment (ED) complaining of acute onset testicular pain. He has vomited twice, but there is no history of any fever or trauma.
Over the past few years, there has been an increase in emergencydepartment (ED) volumes and lengths of stay. The effect of emergencydepartment crowding on lung-protective ventilation utilization for critically ill patients. Paper: Owyang CG, et al. J Crit Care. of patients left the ED on TV settings of 450 mL and 36.1%
In adult trauma cases, there has been significant research to help decide which patients require X-ray or CT imaging for possible cervical spine injuries, leading to the development of the National Emergency X-Ray (NEXUS) prediction rule and the Canadian C-Spine Rule (CCR). What is the problem? What did previous studies show?
Epinephrine – 10ug/mL, 10mL syringe Phenylephrine – 100ug/mL, 10mL syringe Phenylephrine bolus doses from 100-200ug and epinephrine 10-20ug administered every 2-5 minutes pursuant to provider order Inclusion Criteria: Adults age >18 years old Received at least one bolus dose of phenylephrine or epinephrine pre-filled syringes Exclusion (..)
Thanks to the American College of Surgeons and the Institute for Healthcare Improvement, who, along with the American College of Emergency Physicians (ACEP), spearheaded the rule development, the new measure will encourage hospital systems to change the way they approach care for older patients.
The standard care in North America for post-traumatic EDH involves decompressive craniotomy or trepanation via a burr hole, typically performed in an operatingroom by neurosurgery teams. Initially refusing emergency medical services, she was brought to the ED via a private vehicle. The Journal of Emergency Medicine.
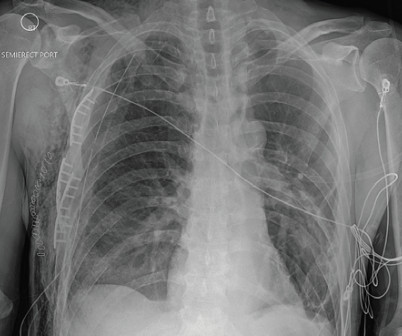
A 58-year-old male with a history of alcohol abuse presented to the emergencydepartment (ED) as a category 2 trauma for a fall with a reported flail chest. His vital signs were within normal limits except for a respiratory rate of 23 with a room air pulse oxygen in the upper 90s. Click to enlarge.)
During Orientations, new crew members must do a minimum of 10 live intubations in the operatingroom before being cleared to intubate in the field. Let’s start with what this study is This study is of a single service with three (3) bases in southeastern Wisconsin and northern Illinois. Data was pulled from June 2013 to June 2018.
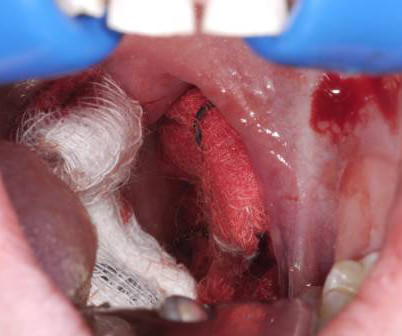
A 24-year-old male with history of quadriplegia and traumatic brain injury presents to the emergencydepartment with hemorrhage in his oral cavity and blood from his tracheostomy tube. 7,8 The significance of this is clear: bronchoscopy or angiography may not suffice to make the diagnosis in the emergency setting.
Date: February 28, 2024 Guest Skeptic: Dr. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Neil Dasgupta is an emergency medicine physician and ED intensivist from Long Island, NY. Case: A 59-year-old man walks into your community emergencydepartment (ED) complaining of chest pain.
4 Pain is the most common reason for presentation in the early post operative period. 5 Highest risk of dislocation early in the post operative course due to laxity of the soft tissue after surgery. 6 Hip flexion or adduction in the early post-operative period can cause atraumatic dislocations (typically avoided for 6 weeks post-op).
EmergeNcyDepartment use of Apneic Oxygenation versus usual care during rapid sequence intubation: A randomized controlled trial (The ENDAO Trial). He writes an excellent […] The post SGEM#186: Apneic and the O, O, O2 for Rapid Sequence Intubation first appeared on The Skeptics Guide to Emergency Medicine.
A search for Brazilian Butt Lift (BBL) on any social media platform will yield thousands of before-and-after images, faja sales, operatingroom videos, recovery tips, and patients praising their plastic surgeon. Or Helly Larson describing the first week after her Miami BBL as “absolute hell” to a Vox reporter.
Diagnosis is clinical and challenged by overlap with more superficial skin infections (i.e. cellulitis) and the need for thorough examination of the genital region. 1 His description of cases of life-threatening infections in the perineal, genital or perianal regions were thought to be idiopathic in previously healthy men.
7 While post-operative adhesive disease is also a risk factor, it is far less commonly implicated in LBO compared to SBO. 7 While post-operative adhesive disease is also a risk factor, it is far less commonly implicated in LBO compared to SBO. He reports distension and the sensation of fullness. Small bowel dilation may also be seen.
A 44 year-old male with unknown past medical history came by emergency medical services (EMS) to the emergencydepartment (ED) for an electrical injury and fall from a high voltage electrical pole. Per EMS, the patient was found at the bottom of a high voltage line with diffuse burns and amputation of his left forearm.
Case A 40-year-old female at 11 weeks, five days gestation presented to the emergencydepartment (ED) with concern for lower abdominal pressure and inability to fully empty her bladder. The patient was admitted to the obstetrics service and underwent spinal anesthesia in the operatingroom to manually reduce the uterus.
C, respiratory rate 20 breaths per minute, and oxygen saturation 95% on room air. 4 This is the framework the ED resuscitationist should be operating under, as hemodynamically unstable pelvic trauma patients require a different approach compared to stable patients who will undergo CT, routine pelvic fixation, and definitive surgical repair.
My first real encounter with the healthcare system took place when I was about seven years old and had to go into hospital for an orchidopexy, so I can empathize with all the young people who come through our emergencydepartment with acute testicular pain. This dropped to 79.3% How do you diagnose torsion? Where does this leave us?
A 28-year-old female G3P2002 presented to the emergencydepartment for one month of vaginal bleeding. The patient was seen in the emergencydepartment one month earlier for vaginal bleeding in the first trimester of pregnancy. Her estimated gestational age was six weeks by last menstrual period.
3 The majority of those who arrive to the emergencydepartment (ED) live for 2 hours or more, leaving a small window for surgical intervention. 3 The majority of those who arrive to the emergencydepartment (ED) live for 2 hours or more, leaving a small window for surgical intervention.
Included patients from out-of-hospital, emergencydepartment, intensive care unit, and operating-room intubations. Intubation performed in all settings (out-of-hospital, emergencydepartment, ICU, and operatingroom). Exclusion criteria: Manikin and cadaver studies. airway scope). to 1.36).
Diagnosis: Diagnosis can be made based on clinical exam alone Physical exam Inability to close the mouth Garbled speech Drooling. Anterior dislocations: palpation of the TMJ can reveal one or both of the condyles to be anteriorly displaced in front of the articular eminence.
Epidemiology Amniotic fluid embolism (AFE) is an incredibly rare yet catastrophic pathology during which fetal debris and/or amniotic fluid enters the maternal central circulation in the third trimester of pregnancy or, most commonly, during the labor process. Regardless, she complains of sudden and severe shortness of breath.
Success at intubation likely takes more time and practice than other procedures, as shown in recent research on ED residents and their success rate at intubating, measured as a function of their total number of intubations (See Figure 1). Practice may not achieve perfection, but it will make you better. fiber optic through the nose).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content