This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
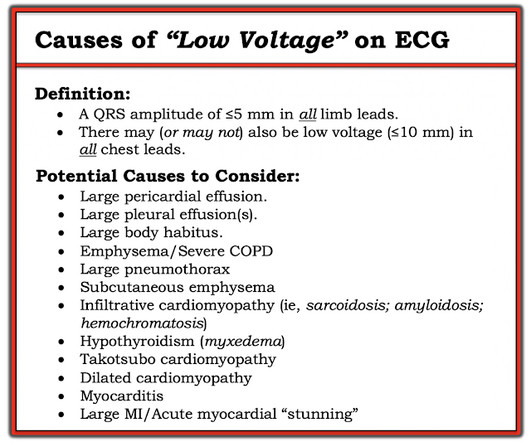
Their OMI Manifesto details how use of standard STEMI criteria results in an unacceptable level of inaccuracy, in which an estimated 25-30% of acute coronary occlusions are missed! The more leads with suspicious findings — the greater the concern for an acute ongoing event.
By Smith, peer-reviewed by Interventional Cardiologist Emre Aslanger Submitted by anonymous A 53 y.o. Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Furthermore, if this occurs at all, it is a rare event. The pain radiated to both shoulders. He was started on nitro gtt.
I published, and Emre Aslanger externally validated, the 4-Variable formula for differentiating the ST Elevation of LAD OMI from Normal ST Elevation. Knowing the patient has a history of coronary disease could be relevant to today's case — as it should add to our suspicion of a new acute event. RED arrows ).
Now let’s compare this with the existing paradigm to identify multiple preventable delays to reperfusion, which can be improved through the paradigm shift from STEMI to OMI. In the STEMI paradigm, patients with ischemic symptoms and ECGs that don’t meet STEMI criteria get serial ECGs.
Takotsubo is a sudden event, not one with crescendo angina. In a prospective angiographic study involving patients undergoing percutaneous intervention for coronary artery disease, only half the subsequent events arose from lesions with sufficient stenosis to have warranted intervention at the time of revascularization. From Gue at al.
Written by Emre Aslanger. Emre is a new Editor of the Blog. I have trouble understanding the chain of events that resulted in the unacceptable delay and cost the patient’s anterior wall. PMID: 34523597. == MY Comment by K EN G RAUER, MD ( 11/13/2022 ): == Highly interesting case by Emre Aslanger. Turk Kardiyol Dern Ars.
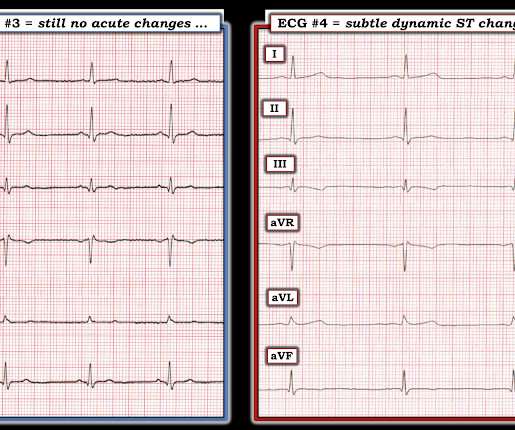
by Emre Aslanger Dr. Aslanger is our newest editorial member. Dr. Aslanger is also the author of the DIFFOCULT study: Emre K. This is a very subtle change but cannot be anything other than an acute coronary event. Take home messages: 1- In STEMI/NSTEMI paradigm you search for STE on ECG. Turk Kardiyol Dern Ars.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content