This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
What are the best options for dosing and administering magnesium sulphate, epinephrine, fentanyl and ketamine in the management of the crashing asthmatic? We answer such questions as: what are the key elements in recognition of threatening asthma? What are the most time-sensitive interventions required to break the vicious cycle of asthma?
Does epinephrine improve the chances of return of spontaneous circulation at the expense of the brain? In other words, while we know that epinephrine doubles rates of ROSC in all comers in cardiac arrest, there’s never been robust evidence for long term improvements in neurologic functional outcomes.
Epinephrine administered intravenously. They administered 10 mcg of push-dose epinephrine. Atropine and further doses of epinephrine were not administered. Paramedics continued compressions and ventilations (30:2 per protocol prior to advanced airway placement) and had an initial rhythm of asystole. Approach TCP with skepticism.
Nick Clarridge runs through the NRP algorithm and delivers the nuggets of wisdom on when and how best to perform chest compressions, give epinephrine and pearls and pitfalls of the algorithm.
Chris Root is an emergency medicine and emergency medicine service (EMS) physician at the University of New Mexico, Albuquerque. Chris completed his emergency medicine residency and EMS fellowship at UNM. Before attending medical school, he was a New York City Paramedic. There is drug paraphernalia scattered around the room.
Date: January 11, 2024 Guest Skeptic: Dr. Chris Root is an EMS fellow in the Department of Emergency Medicine at the University of New Mexico Health […] The post SGEM#426: All the Small Things – Small Bag Ventilation Masks in Out of Hospital Cardiac Arrest first appeared on The Skeptics Guide to Emergency Medicine. Resuscitation 2023.
The post EM Quick Hits 12 AFib Early vs Delayed Cardioversion, Snake Bites, Ovarian Torsion Myths, Crystal Meth, Aortic Dissection, Severe Asthma Meds appeared first on Emergency Medicine Cases.
To celebrate the end of trauma season ( is it ever really over? ), we here at the Ped EM Morsels Bakery have cooked up a morsel to remind you that pediatric trauma can be even more difficult than you think. Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Never fear.
to 0.5mg (1mg/mL) IV Bolus: 5 to 20mcg (10mcg/mL) IV Infusion: 1 to 20mcg/min If Poor Response to Conventional Therapy Consider Epinephrine 100mcg IV bolus Norepinephrine infusion 0.1mcg/kg/min Vasopressin 0.01
How Long Should We Monitor After Giving IM Epinephrine for Anaphylaxis? Bottom Line Up Top: After prompt recognition and appropriate treatment with IM epinephrine, the risk of biphasic reactions are exceedingly low. At the time of discharge, appropriate patient education and prescriptions for IM epinephrine are essential.
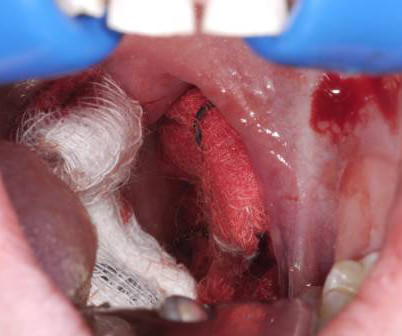
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression.
A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. You are the first provider on scene with Emergency Medical Services (EMS) and start high-quality Cardiopulmonary Resuscitation (CPR). Date: December 6th , 2018 Reference: Perkins et al.
WE, AS EMS PROFESSIONALS, SHALL PROVIDE COMPASSIONATE, APPROPRIATE CARE TO ALL PATIENTS. EMS must rely on the hazmat team to monitor the air and not rely on their sense of smell. Children who develop stridor may be treated with racemic epinephrine (0.25- 0.75ml of 2.25% racemic epinephrine to 2.5
JAMA 2020 Guest Skeptic: Mike Carter is a former paramedic and current PA practicing in pulmonary and critical care as well as an adjunct professor of emergency medical services […] The post SGEM#314: OHCA – Should you Take ‘em on the Run Baby if you Don’t get ROSC? first appeared on The Skeptics Guide to Emergency Medicine.
He is an EMS medical director with Lexington Fire/EMS as well as the AMR/NASCAR […] The post SGEM#329: Will Corticosteroids Help if…I Will Survive a Cardiac Arrest? He is an EMS medical director with Lexington Fire/EMS as well as the AMR/NASCAR Safety Team. first appeared on The Skeptics Guide to Emergency Medicine.
We’ll keep it short, while you keep that EM brain sharp. 2][3] Bacterial tracheitis should be suspected over croup if nebulized racemic epinephrine or steroids do not improve the clinical course. [2][3][8] link] The post EM@3AM: Bacterial Tracheitis appeared first on emDOCs.net - Emergency Medicine Education. 1983;137(8):764.
In anticipation of EM Cases Episode 112 on Tachydysrhthmias with Amal Mattu and Paul Dorion, Melanie Baimel tells her Best Case Ever of a previously healthy young man who presents in refractory ventricular fibrillation after receiving multiple single shocks, ongoing chest compressions, several rounds of epinephrine, amiodarone and dual sequence defibrillation (..)
After administering 1mg of epinephrine ROSC is noted with a bradycardic rhythm ( Figure 2 ). Two paramedics are in the rear of the ambulance managing resuscitation (another crew had arrived and provided support with a driver). During transport, the paramedic not dedicated to compressions is able to establish IV access in the patient's hand.
Case: You are the Chief of your local Fire and EMS Department, and an individual contacts you saying […] The post SGEM#380: OHCAs Happen and You’re Head Over Heels – Head Elevated During CPR? Head and thorax elevation during cardiopulmonary resuscitation using circulatory adjuncts is associated with improved survival.
Case: An EMS crew arrives at the home of a 68-year-old suffering from a witnessed out-of-hospital cardiac arrest (OHCA). Intraosseous access is quickly obtained, and a dose of epinephrine is provided. JAMA 2021 This was an SGEM Journal Club and all the slides from the presentation can be downloaded using this LINK.
She is the host of EM Bootcamp in Las Vegas, as well as a usual speaker and faculty member for The Center for Continuing Medical Education (CCME). She is the host of EM Bootcamp in Las Vegas, as well as a usual speaker and faculty member for The Center for Continuing Medical Education ( CCME ). Reference: Vent et al. lumbar punctures).
We discuss that the palpation technique is poor at determining whether or not a patient has a pulse, that the POCUS pulse is more accurate and as rapid compared to the palpation technique at determining whether or not a patient has a pulse, the difference between true PEA arrest, PseudoPEA and PREM, why epinephrine may be harmful in PEA, Weingart's (..)
Soak the gauze with epinephrine (1:10,000) or TXA (our THIRD route of administration) Apply pressure laterally to the tonsillar fossa with the gauze covered Magill forceps. The post Post-Tonsillectomy Hemorrhage: ReBaked Morsel appeared first on Pediatric EM Morsels. Don’t await for fancy meds to arrive from pharmacy.
The post EM Quick Hits 35 – 10 Best Papers of 2021, Peripartum Cardiomyopathy, Crashing Asthmatic, Febrile Neutropenia, Anaphylaxis update appeared first on Emergency Medicine Cases.
Earlier in the year, we released the 2024 ESO EMS, Fire Service, and Hospital Trend Reports , which forecasted the trends ESO experts believed would shape each industry. With contributions from over 2,700 EMS agencies, fire departments, and hospitals across the U.S., This year, we released When Do Minutes Matter?
In this first part of our 2-part series on Cardiac Arrest Controversies Rob Simard, Bourke Tillman, Sara Gray and Scott Weingart discuss with Anton how best to ensure high quality chest compressions, the pros and cons of mechanical CPR, the literature on dual sequential defibrillation and optimizing pad placement, epinephrine vs vasopressin, amiodarone (..)
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine.
1: Epinephrine or Airway First in OHCA? Spoon Feed In adults presenting to EMS after OHCA, those receiving epinephrine prior to advanced airway management (AAM = supraglottic airway, SGA, or endotracheal tube) experienced better outcomes and prehospital ROSC than those receiving AAM before epinephrine. JAMA Netw Open.
Yet at the same time, despite a large-scale Holmberg study involving over 6,000 patients suggesting potential harm, epinephrine remained part of the pediatric symptomatic bradycardia protocol. EMS is a unique subspecialty within medicine, and we owe it to our patientsand to ourselvesto dig deeper. By now, you can see the pattern.
Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh. 2020) The Times & Tapes Are a-Changin’: The Latest Broselow-Luten Tape for EMS , EMS World.
Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a critical care paramedic and first year medical student at Rocky Vista University in Colorado. Annals of EM May 2018 Guest Skeptic: Andrew Merelman is a critical care paramedic and first year medical student at Rocky Vista University in Colorado.
” If the patient has compromise to airway, breathing or circulation, they should get immediate epinephrine. In anaphylaxis, think, “If A, B or C, give E.” D-dimer can effectively rule out a larger portion of low risk patients if age adjustment or the YEARS criteria are employed.
EMS arrived and found him in Ventricular Fibrillation (VF). After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% This patient was witnessed by bystanders to collapse. They started CPR. He was defibrillated into VT. sodium bicarbonate.
Case: You are the medical director of an EMS system in a large city deciding on whether to respond to all out of hospital cardiac arrests (OHCA) with ACLS capabilities, or if resources should be directed to those candidates for extracorporeal CPR. You need to recognize an arrest and activate your EMS system. vs. 66.8%, p=0.73).
Date: April 4th, 2020 It has been just over a year since Dr. Salim Razaie (REBEL EM) and I stepped into the ring for a boxing matched theme debate in Sydney, Australia. Date: April 4th, 2020 It has been just over a year since Dr. Salim Razaie ( REBEL EM) and I stepped into the ring for a boxing matched theme debate in Sydney, Australia.
Alongside his EM residency, he is doing a PhD in epidemiology. Alongside his EM residency, he is doing a PhD in epidemiology. The first visit was back in 2013 for SGEM#50 : Under Pressure – Vasopressin, Steroids and Epinephrine in Cardiac Arrest. Robert’s academic interests include research and evidence-based medicine.
He is also part of REBEL EM, The Teaching Course, […] The post SGEM#188: Icatibant Bites the Dust – For ACE-I Induced Angioedema first appeared on The Skeptics Guide to Emergency Medicine. He is also part of REBEL EM , The Teaching Course , EMRAP and CoreEM. display_podcast] Date: September 12th, 2017 Reference: Sinert et al.
Dan recaps the MD1 EMS Conference and shares what he learned from a room full of EM/EMS physicians speaking to EMS clinicians! link] Ultrasound in Cardiac Arrest: [link] Happy EMS Week! We're heading to the MD1/EMS and Disaster Medicine Fellowship Conference at Newark Beth Israel Medical Center!
Case: EMS arrive to your emergency department with a 68-year-old man post cardiac arrest patient. There is no evidence for a patient-oriented benefit with epinephrine ( SGEM#238 ), other ACLS drugs ( SGEM#64 ), pre-hospital therapeutic hypothermia ( SGEM#54 , SGEM#183 ), or mechanical CPR ( SGEM#136 ).
In the fast-paced world of emergency medical services (EMS), precision in pediatric medication dosing can mean the difference between life and death. The Monroe-Livingston Regional EMS (MLREMS) has spearheaded a transformative approach that ensures the safest and most effective treatment for our youngest patients during emergency situations.
Authors: Alex Rogers, MD (EM Resident Physician, Christus Spohn/Texas A&M University School of Medicine, Corpus Christi, TX); J.D. 1,2] Consider using a physiological marker to help identify inadvertent vascular injection, such as epinephrine. [3] If epinephrine is used, small initial doses ( <1 ug/kg) are preferred.
Talk Trauma is a two-day conference for nurses, allied health and EMS professionals involved in providing care for the adult and paediatric trauma patient. Case: A 52-year-old man presents to the emergency department via EMS after a motor vehicle collision while driving home from the city. You suspect he has been drinking.
In cardiac arrest, a delay in IV access subsequently results in a delay in epinephrine administration. Rezaie, MD (Twitter/X: @srrezaie ) The post Don’t Forget About the IO in the Critically Ill Patient appeared first on REBEL EM - Emergency Medicine Blog.
Authors: Christian Gerhart, MD (EM Resident Physician, Washington University in St. Louis); Dr. Jessica Pelletier, DO (EM Attending Physician, Washington University in St. You receive a page for a cardiac arrest and take report from emergency medical services (EMS). Per EMS he was very cold to touch. 2009;338:b2085.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content