This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse McLaren illustrates the paradigm shift from STEMI to Occlusion MI (OMI) through 9 cases, and drives home the points that if there is STEMI criteria, consider false positives (eg. secondary and proportional to LVH or BER); if there is no STEMI criteria, consider false negatives and look for other signs of occlusion (eg.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Upon EMS arrival, they find the patient is sweaty with normal vital signs. AEM November 2023.
Can you identify which were early repolarization and which were anterior STEMI? The post ECG Cases 2: Early Repolarization or Anterior STEMI? In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. appeared first on Emergency Medicine Cases.
And for STEMI too. The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. Does heparin - LMWH or unfractionated heparin - benefit the patient with a pretty good story for angina with a bump in their troponin and some ST depression in the lateral leads? But should we? But should we?
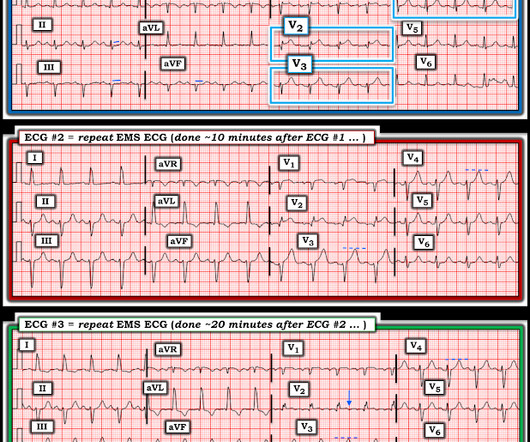
Written by Pendell Meyers A woman in her 70s had acute chest pain and called EMS. On arrival, EMS recorded relatively normal vital signs and this EMS ECG: What do you think? The EMS crew recorded another ECG about 10 minutes later (unknown if pain changed): New LAFB. So the cath lab was not activated. Ongoing OMI.
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
We consider electrolyte disturbances and look for ECG signs of hyperkalemia or hypokalemia/hypomagnesemia, and we consider the differential of diffuse ST depression with reciprocal ST elevation in aVR, and false positive STEMI.
For instance, there was no protocol for stroke or STEMI. At some point along the way we had protocols for spinal motion restriction, alcohol withdrawal, stroke and STEMI, CPAP, and termination of cardiac arrest resuscitation on scene. There were fewer than 50 protocols in the book, along with pages for 24 medications and 8 procedures.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" He diagnosed anterior "STEMI" and activated the cath lab. What do you think? But he did well.
He called EMS who brought him to the ED. She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. And the pace only quickens.
Metropolitan Emergency Medical Services (MEMS) is a public, non-profit EMS entity serving Little Rock, Arkansas, and its surrounding counties. In 2020, MEMS adopted Pulsara to improve communication with area hospitals for time-sensitive emergencies such as stroke, STEMI, and trauma. MEMS transports around 77,000 patients each year.
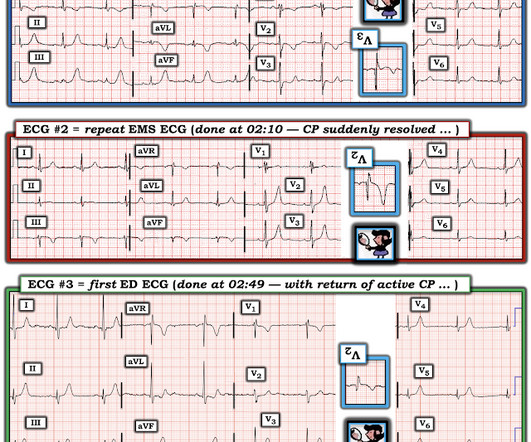
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? Now let’s look at the actual sequence, with the addition of clinical context, and see how the patient was managed: The patient received aspirin from EMS and arrived at triage painfree (ECG #1). 2 Normal ECG #3.
Jason was very skeptical of STEMI. This also argues against STEMI. Turns out that the patient regularly called EMS for complaints of chest pain that frequently led to cath lab activation.) He complained of 3 days of diarrhea and abdominal pain. What do you think? Jason, I agree. V4 especially looks like early repolarization.
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration.
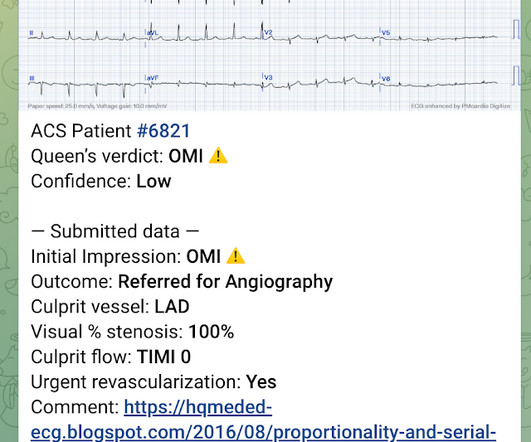
Written by Jesse McLaren A previously healthy 60 year old developed exertional chest pain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
From April 2-5, the top fire services and EMS industry thought leaders and data analysts gathered at Wave 2024 to share what trends they’re forecasting for both fields and how they’re enacting change within their own organizations through the power of data-driven insights. Data impacts every aspect of duties, from shifts start to end.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
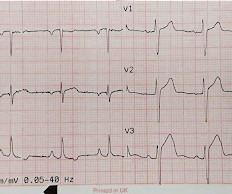
LVH produces secondary repolarization abnormalities that can mimic STEMI. Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. In this case, the EMS provider was routed to the urgent care facility.
Episode 86: Tricky Cases Part 2 Case 3: 56-year-old female with history of seizures, actively seizing, EMS called. Patient seized for approximately 20 minutes prior to EMS arrival. Today on the emDOCs cast with Brit Long, MD ( @long_brit) , and Rachel Bridwell, MD ( @rebridwell ), we cover two more challenging cases.
EMS was called to evaluate a male patient in his 60s with a chief complaint of chest pain. Onset: Gradual while walking Provoke: Initially the pain felt better with rest Quality: Described as a dull ache Radiate: The pain radiates to the back Severity: 7/10 Time: 3 hours He states that he feels nauseated and vomited x2 prior to EMS arrival.
His initial EKG is the following: What do you think? Naturally you would assume that this was a large, multicenter trial, right? This was based on 11, thats not a typo, ELEVEN patients. Ok, so what did the PROCAMIO trial find? Ok, so what did the PROCAMIO trial find? Well, the trial was a multicenter prospective open label trial.
Fire/EMS crews found him clammy and uncomfortable. It doesn’t meet any conventional STEMI criteria, but there is patently obvious increased area under the curve. Vital signs were noted to be unremarkable with respect to any hypo-hypertensive crisis, hypoxia, etc. Breath sounds were clear in all lung fields. No appreciable skin pallor.
He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic. The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”. The ST depressions in I and aVL have resolved.
Written by Pendell Meyers A middle aged man called EMS for acute chest pain. EMS recorded this ECG during active symptoms and transmitted it to the ED: I had no information when I was shown the ECG. I believe there is not quite enough STE for formal STEMI criteria, but some might measure 1.0 I said "Not OMI.
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chest pain. They explain complementary diagnostic insights into pericardial effusion and cardiac tamponade, occlusion MI and RV strain.
According to the EMS narrative, this patient initially refused hospital transport and advised that he would seek evaluation at a later time with his personal physician. A prehospital STEMI activation was transmitted to the closest PCI center, and 324mg ASA was administered. A 12 Lead ECG was recorded. A 12 Lead ECG was recorded.
Written by Bobby Nicholson What do you think of this “STEMI”? With EMS, patient had a GCS of 3 and was saturating 60% on room air. He improved to 100% with the addition of non-rebreather, however remained altered and was intubated by EMS with ketamine and succinylcholine. or basilar ischemia. There is high QRS voltage.
Written by Pendell Meyers I received this prehospital ECG (we receive prehospital ECGs by telemetry from EMS in a large area around our hospital) and was told that there was a patient in her 50s with chest pain who was headed to an outside hospital (which happens to be a catheterization center). Here is the ECG: What do you think?
Generally speaking, right bundle branch block does not mimic, or obscure, the ECG diagnosis of acute STEMI the way left bundle branch block does. Case Review EMS is called to the residence of a 69 y/o M with a chief complaint of chest pain. Concept Review How do you identify right bundle branch block (RBBB) on the 12 lead ECG?
A 60-something woman called EMS for chest pain. Waiting to cath a transient STEMI can be hazardous. This case comes from Jason Winter, of The Facebook Clinical Electrocardiology ECG Page. Here is her first prehospital ECG: What do you think? There is very low voltage in the precordial leads, with a total QRS amplitude of only 3.5
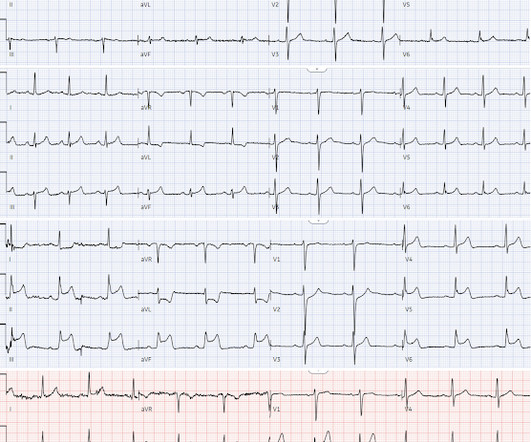
There’s inferior ST depression which is reciprocal to subtle lateral convex ST elevation, and the precordial T waves are subtly hyperacute – all concerning for STEMI(-)OMI of proximal LAD. There’s ST elevation I/aVL/V2 that meet STEMI criteria. This is obvious STEMI(+)OMI of proximal LAD. Non-STEMI or STEMI(-)OMI?
EMS arrived and found him in Ventricular Fibrillation (VF). Cardiac arrest #3: ST depression, Is it STEMI? This patient was witnessed by bystanders to collapse. They started CPR. He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. After 1 mg of epinephrine they achieved ROSC.
Fire/EMS personnel find her laying supine on the kitchen floor, awake and verbal, although acutely ill. This worried the crew of potential acute coronary syndrome and STEMI was activated pre-hospital. As it currently stands, an ST/S ratio >15% should raise awareness for new anterior STEMI.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
EMS arrived and recorded this ECG: What do you think? Notice on the right side of the image how the algorithm correctly measures STE sufficient in V1 and V2 to meet STEMI criteria in a man older than age 40. As most would agree, this ECG shows highly specific findings of anterolateral OMI, even with STEMI criteria in this case.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Do either, both, or neither have occlusion MI? Vitals were normal.
He had multiple cardiovascular risk factors and the EM physician strongly suspected ACS. Over the next few hours, four other general cardiologists "signed off on the initial ECG without recognizing STEMI." Learning Points: STEMI criteria misses 25-40% of OMI, like this case for example. mm of the "required" 1.0
He has a history of STEMI and heart failure. link] Case continued The conventional algorithm diagnosed STEMI and so did the paramedics. A Coronary angiogram from 8 years prior revealed that he had had an inferior posterior STEMI at the time due to 100% occlusion of the proximal RCA. A 50-something had syncope while driving.
EMS arrived and recorded vital signs within normal limits and the following ECG during active pain: EMS1 @ 0157: What do you think? Unfortunately you can see that the conventional Zoll algorithm sees nothing even to suggest AMI, let alone STEMI. During EMS transport, the pain suddenly resolved.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content