This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse McLaren illustrates the paradigm shift from STEMI to Occlusion MI (OMI) through 9 cases, and drives home the points that if there is STEMI criteria, consider false positives (eg. secondary and proportional to LVH or BER); if there is no STEMI criteria, consider false negatives and look for other signs of occlusion (eg.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
How can we use the awareness of complications to identify false positive STEMI and Occlusion MI that doesn’t meet classic STEMI criteria, and consider specific treatment? The post ECG Cases 41 – STEMI, Occlusion MI Complications appeared first on Emergency Medicine Cases.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Upon EMS arrival, they find the patient is sweaty with normal vital signs. AEM November 2023.
The post EM Quick Hits 4 Acetaminophen Overdose & Warfarin Interaction, Dental Infections, MTP RABT Score, Statins for STEMI, Cricothyrotomy Tips appeared first on Emergency Medicine Cases.
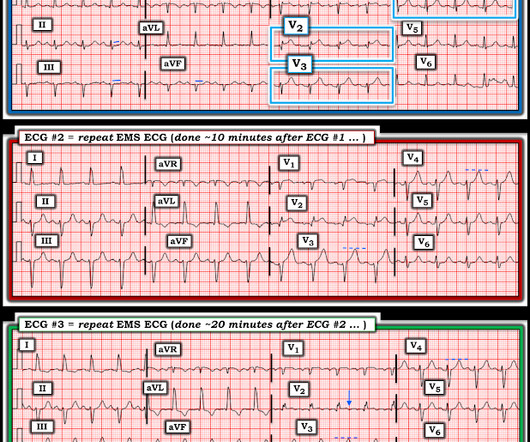
Written by Pendell Meyers A woman in her 70s had acute chest pain and called EMS. On arrival, EMS recorded relatively normal vital signs and this EMS ECG: What do you think? The EMS crew recorded another ECG about 10 minutes later (unknown if pain changed): New LAFB. So the cath lab was not activated. Ongoing OMI.
And for STEMI too. The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. We’re expected to routinely give heparin for all these NSTEMI and unstable angina patients with any ischemic changes seen on the ECG, right? But should we?
Can you identify which were early repolarization and which were anterior STEMI? The post ECG Cases 2: Early Repolarization or Anterior STEMI? In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. appeared first on Emergency Medicine Cases.
In this ECG Cases blog we look at 9 patients with possible transient STEMI and discuss pitfalls and pearls in ECG interpretation and management. The post ECG Cases 39 – Transient STEMI Pitfalls and Pearls appeared first on Emergency Medicine Cases.
10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. The post ECG cases 7: ST elevation in aVR, STEMI-equivalent? Which had acute coronary occlusion? Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog.
Background: Primary PCI is the recommended reperfusion strategy in patients with STEMI and should be initiated within 2 hours after first medical contact. In non-PCI-capable hospitals this goal is not always achievable due to delays in transfer. In these cases, thrombolysis is recommended to improve morbidity and mortality. Primary PCI: 95.7%
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
Jesse McLaren explains 'Late STEMI' and how reperfusion strategies should not be based on time of symptom onset. The post ECG Cases 25: ‘Late STEMI’ – How acute is the coronary occlusion? In this ECG Cases blog we look at 10 patients with potentially ischemic symptoms. appeared first on Emergency Medicine Cases.
Written by Pendell Meyers A man in his 40s called EMS for acute chest pain that awoke him from sleep, along with nausea and shortness of breath. Learning Points: Currently by definition, there is unfortunately no such thing as a formal diagnosis of STEMI or STEMI criteria in the setting of RBBB and LAFB.
The post EM Quick Hits 50 Normal Unenhanced CT Renal Colic DDx, Perichondritis, Magnesium in Pediatric Asthma, Steroids for Pneumonia, OMI Cath Lab Activation appeared first on Emergency Medicine Cases.
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
For instance, there was no protocol for stroke or STEMI. At some point along the way we had protocols for spinal motion restriction, alcohol withdrawal, stroke and STEMI, CPAP, and termination of cardiac arrest resuscitation on scene. The book was approved by the two largest hospitals in Hartford. Paramedics didnt do 12-lead ECGs then.
We consider electrolyte disturbances and look for ECG signs of hyperkalemia or hypokalemia/hypomagnesemia, and we consider the differential of diffuse ST depression with reciprocal ST elevation in aVR, and false positive STEMI. The post ECG Cases 44 ECG Interpretation in Epigastric pain, Vomiting appeared first on Emergency Medicine Cases.
Metropolitan Emergency Medical Services (MEMS) is a public, non-profit EMS entity serving Little Rock, Arkansas, and its surrounding counties. In 2020, MEMS adopted Pulsara to improve communication with area hospitals for time-sensitive emergencies such as stroke, STEMI, and trauma. MEMS transports around 77,000 patients each year.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Post Created By: William Caputo MD Post Peer Reviewed By: Anand Swaminathan MD, MPH (Twitter @EMSwami ) The post REBEL Core Cast 104.0 – Subtle ECGs in Acute Coronary Occlusion appeared first on REBEL EM - Emergency Medicine Blog.
Systematically developed statements to assist Dr and patient e.g. trauma calls, STEMI pathways, drug Pros Use of effective treatment Consistent … Continue reading →
From April 2-5, the top fire services and EMS industry thought leaders and data analysts gathered at Wave 2024 to share what trends they’re forecasting for both fields and how they’re enacting change within their own organizations through the power of data-driven insights. Data impacts every aspect of duties, from shifts start to end.
EMS personnel found him seated on a bench, uncomfortable, but without gross distress. A third, and final, EMS 12 Lead ECG was recorded: The precordial ST segments (even Leads I/aVL, as well) have reverted to a dramatically depressed state. it has been subsequently deemed a STEMI-equivalent.
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? Now let’s look at the actual sequence, with the addition of clinical context, and see how the patient was managed: The patient received aspirin from EMS and arrived at triage painfree (ECG #1).
His family started CPR and called EMS, who arrived to find him in ventricular fibrillation. 15 minutes after EMS arrival, after at least 6 defibrillations, the patient achieved sustained ROSC. Written by Pendell Meyers A man in his 50s was found by his family in cardiac arrest of unknown duration.
Written by Jesse McLaren A previously healthy 60 year old developed exertional chest pain with diaphoresis, and called EMS. Here’s the EMS ECG, digitized with PM cardio. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
In this month's EM Quick Hits podcast: Anand Swaminathan on lateral canthotomy, Emily Austin on pediatric cannabis poisoning, Reuben Strayer on an approach to hyperthermia, Brit Long on diagnosis and management of malignant otitis externa, Jesse McLaren on ECG diagnosis of occlusion MI in patients with BBB and Peter Brindley on prone CPR.
In this ECG Cases blog we review 8 cases of patients with prehospital ECGs and explore prehospital ECGs for diagnosing STEMI, Occlusion MI, false STEMI, code STEMI, dynamic ischemic changes, truncated voltages. Can you avoid the pitfalls and spot the pearls that help to make the diagnosis?
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
Written by Pendell Meyers Two adult patients in their 50s called EMS for acute chest pain that started within the last hour. Both cases had an EMS ECG that was transmitted to the ED physician asking "should we activate the cath lab?" He diagnosed anterior "STEMI" and activated the cath lab. What do you think? But he did well.
In patients with chest pain + ST elevation, consider false positive STEMI including early repolarization, LVH and Brugada-pattern. In patients with cocaine chest pain who are STEMI negative, beware STEMI(-)OMI including subtle ST elevation, hyperacute T waves, reciprocal change, and refractory ischemia.
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
EMS was called to evaluate a male patient in his 60s with a chief complaint of chest pain. Onset: Gradual while walking Provoke: Initially the pain felt better with rest Quality: Described as a dull ache Radiate: The pain radiates to the back Severity: 7/10 Time: 3 hours He states that he feels nauseated and vomited x2 prior to EMS arrival.
The PEC Podcast with host Dr. Maia Dorsett brings you our Deep Dive Series with: Daniel Joseph MD Kevin Burns EMT-P, PA-C Aman Shah MD who discuss their manuscript: STEMI Equivalents and Their Incidence during EMS Transport Click here to download today! As always THANK YOU for listening.
In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, none of whom had STEMI on the 12 lead ECG. Which had occlusion MI? The post ECG cases 6: Posterior MI – Still Under-recognized appeared first on Emergency Medicine Cases.
Written by Pendell Meyers A woman in her 30s called EMS for acute symptoms including near-syncope, nausea, diaphoresis, and abdominal pain. EMS arrived and found her to appear altered, critically ill, and hypotensive. EMS reportedly gave 4 grams of calcium (unknown whether CaCl or gluconate) and 50 mEq of sodium bicarbonate.
Seven patients with ischemic symptoms, none meeting STEMI criteria but all identified by a specific pattern of first diagonal branch occlusion are explored in this ECG Cases blog with Jesse MacLaren who also explains The South African Flag Sign.
EMS was called, and they recorded the following ECG on scene at 13:16: What do you think? In this medical system, the EMS provider can then be routed to the ED or to a type of urgent care facility that is open 24 hrs/day and staffed by a primary care provider. In this case, the EMS provider was routed to the urgent care facility.
He reported to EMS a medical history of GERD only. BP 142/100 HR 90 RR 16 (BBS CTA) SpO2 99 (RA) Dstick 110 My colleagues noted the ST-depression in the respective leads, as well, and STEMI activated to the nearest PCI center. 1] Here is the admitting ED ECG after cancellation of Code STEMI. However, in this context (i.e.
LVH produces secondary repolarization abnormalities that can mimic STEMI. Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves.
Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. Guest Skeptic: Dr. Stephen Meigher is the EM Chief Resident training with the Jacobi and Montefiore Emergency Medicine Residency Training Program. The TOMAHAWK Investigators.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content