This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Does epinephrine improve the chances of return of spontaneous circulation at the expense of the brain? In other words, while we know that epinephrine doubles rates of ROSC in all comers in cardiac arrest, there’s never been robust evidence for long term improvements in neurologic functional outcomes.
A pre-post study conducted in North Carolina compared multi-dose epinephrine with single-dose epinephrine in adult non-traumatic out-of-hospital cardiac arrest (OHCA) patients. Link to article
Epinephrine and cardiac arrest: what’s the question? How much epinephrine is enough? published a retrospective study in AJEM discussing cumulative epinephrine dosage in cardiac arrest. Garcia et al.
Epinephrine administered intravenously. They administered 10 mcg of push-dose epinephrine. Atropine and further doses of epinephrine were not administered. Paramedics continued compressions and ventilations (30:2 per protocol prior to advanced airway placement) and had an initial rhythm of asystole. Approach TCP with skepticism.
What are the best options for dosing and administering magnesium sulphate, epinephrine, fentanyl and ketamine in the management of the crashing asthmatic? We answer such questions as: what are the key elements in recognition of threatening asthma? What are the most time-sensitive interventions required to break the vicious cycle of asthma?
Nick Clarridge runs through the NRP algorithm and delivers the nuggets of wisdom on when and how best to perform chest compressions, give epinephrine and pearls and pitfalls of the algorithm.
Consider these medications if there are signs of end-organ dysfunction, there is a considerable delta in baseline BP, systolic is less than 90 and/or MAP is less than 65 Norepinephrine is a good pressor for a lot of the situations that we encounter in the emergency department, such as septic shock, undifferentiated shock and hypovolemic shock.
How Long Should We Monitor After Giving IM Epinephrine for Anaphylaxis? Bottom Line Up Top: After prompt recognition and appropriate treatment with IM epinephrine, the risk of biphasic reactions are exceedingly low. At the time of discharge, appropriate patient education and prescriptions for IM epinephrine are essential.
to 0.5mg (1mg/mL) IV Bolus: 5 to 20mcg (10mcg/mL) IV Infusion: 1 to 20mcg/min If Poor Response to Conventional Therapy Consider Epinephrine 100mcg IV bolus Norepinephrine infusion 0.1mcg/kg/min Vasopressin 0.01
Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Crystalloid may help, but neurogenic shock may not respond to fluid administration. Alpha 1 agonists are necessary to maintain appropriate blood pressure.
Initial Management After a rapid assessment, we inserted an anterior nasal pack, soaked in epinephrine, TXA, and an antibiotic-based lubricant. We report a case of a 50-year-old man with end stage renal disease with massive nasal bleeding from the left nostril, shortness of breath, and confusion.
You and your partner initiate high-quality CPR, place a supraglottic airway, establish intra-osseous (IO) access and administer epinephrine. There is drug paraphernalia scattered around the room. Your partner asks if you want to administer naloxone as well.
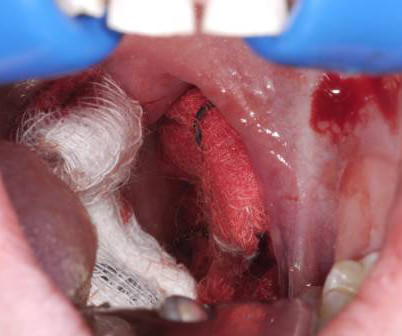
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression.
A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. An oral airway is placed, peripheral intravenous (IV) line started successfully and the paramedic asks her partner if you want to administer IV epinephrine? He is unsuccessfully shocked.
After administering 1mg of epinephrine ROSC is noted with a bradycardic rhythm ( Figure 2 ). Two paramedics are in the rear of the ambulance managing resuscitation (another crew had arrived and provided support with a driver). During transport, the paramedic not dedicated to compressions is able to establish IV access in the patient's hand.
University of Maryland Department of Emergency Med
OCTOBER 11, 2023
1,2 Epinephrine autoinjector. Background: It is estimated that nearly 6% of U.S. adults and children report having a food allergy.1,2 Click to view the rest
In this first part of our 2-part series on Cardiac Arrest Controversies Rob Simard, Bourke Tillman, Sara Gray and Scott Weingart discuss with Anton how best to ensure high quality chest compressions, the pros and cons of mechanical CPR, the literature on dual sequential defibrillation and optimizing pad placement, epinephrine vs vasopressin, amiodarone (..)
The post EM Quick Hits 12 AFib Early vs Delayed Cardioversion, Snake Bites, Ovarian Torsion Myths, Crystal Meth, Aortic Dissection, Severe Asthma Meds appeared first on Emergency Medicine Cases.
Intraosseous access is quickly obtained, and a dose of epinephrine is provided. Bystander CPR is being performed. The monitor is hooked up. The paramedics performed high-quality CPR and follow their ACLS protocol. CPR is continued while a supraglottic airway is placed successfully.
SGEM#50 looked at a RCT published in JAMA 2013 looking to see if a vasopressin, steroids, and epinephrine (VSE) protocol for IHCAs could improve survival with favorable neurologic outcome compared to epinephrine alone. I have not seen a validation study published.
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine.
Resuscitation recently published an article that assessed the association between intramuscular (IM) epinephrine and survival outcomes, including survival to hospital discharge, survival to hospital admission, and functional survival. Link to article
HIET improves contractility without increasing SVR, while vasopressin and epinephrine transiently increase SVR/MAP but worsen cardiac output in anesthetized dogs given propranolol (Holger 2007). Insulin versus vasopressin and epinephrine to treat β-blocker toxicity. Strong trend across different study designs for superiority of HIET.
Buffered lidocaine 1%, epinephrine 1:100,000 with sodium bicarbonate (hydrogencarbonate) in a 3:1 ratio is less painful than a 9:1 ratio: A double-blind, randomized, placebo-controlled, crossover trial. Epinephrine in Local Anesthetics: This will not make the tip of things fall off (nose, fingers, toes, etc). Reference: Vent et al.
Children who develop stridor may be treated with racemic epinephrine (0.25- 0.75ml of 2.25% racemic epinephrine to 2.5 Consider nebulized bronchodilators for bronchospasm, using the standard cautions in their use based on the age of the patient.
Intensive Care Medicine recently published an article with focus on “Epinephrine versus norepinephrine in cardiac arrest patients with post-resuscitation shock” This study was in Paris metropolitan region. The choice of vasopressor is always a topic of controversy regarding post cardiac arrest patients.
This includes epinephrine for OHCA, target temperature management, mechanical CPR, supraglottic airways, steroids, hands on defibrillation and many more topics. Background: We have covered Out of Hospital Cardiac Arrests (OHCAs) many, many times on the SGEM.
We discuss that the palpation technique is poor at determining whether or not a patient has a pulse, that the POCUS pulse is more accurate and as rapid compared to the palpation technique at determining whether or not a patient has a pulse, the difference between true PEA arrest, PseudoPEA and PREM, why epinephrine may be harmful in PEA, Weingart's (..)
1: Epinephrine or Airway First in OHCA? Spoon Feed In adults presenting to EMS after OHCA, those receiving epinephrine prior to advanced airway management (AAM = supraglottic airway, SGA, or endotracheal tube) experienced better outcomes and prehospital ROSC than those receiving AAM before epinephrine. JAMA Netw Open.
Soak the gauze with epinephrine (1:10,000) or TXA (our THIRD route of administration) Apply pressure laterally to the tonsillar fossa with the gauze covered Magill forceps. . < 25 kg = 250 mg up to 3x > 25 kg = 500 mg up to 3x Direct Pressure Always the best way to stop bleeding. Don’t await for fancy meds to arrive from pharmacy.
Epinephrine is provided and you quickly place an advanced airway. A second dose of epinephrine is given, and you start to think about reversible causes and your next steps for in-hospital cardiac arrests (IHCA). Cardiopulmonary resuscitation (CPR) is in progress. The monitor shows a non-shockable rhythm.
Vasopressor medications during cardiac arrest We recommend that epinephrine be administered for patients in cardiac arrest. It is reasonable to administer epinephrine 1 mg every 3 to 5 minutes for cardiac arrest. High-dose epinephrine is not recommended for routine use in cardiac arrest. COR 1, LOE B-R. COR 2a, LOE B-R.
Read the 2024 ESO EMS Index Read the 2024 ESO Fire Service Index Post-Resuscitation Epinephrine Vs. Norepinephrine in Cardiac Arrest Released in May 2024 Epinephrine and norepinephrine are both commonly used as prehospital vasopressors in the United States.
. #2: Treat bradycardia Calcium: 1 g calcium chloride or 3 g calcium gluconate IV; redosing is often necessary Epinephrine: 5-10 mcg/minute Will improve heart rate and shift potassium intracellularly If still unstable after calcium and epinephrine, pacing will be needed Skip atropine #3: Treat hyperkalemia If thinking BRASH, start hyperkalemia treatment (..)
Removal: Lokelma (Sodium Zirconium cyclosilicate) Luckily residents have never had to use Kayexalate Can start working in 1-2 hours of administration 0.37
After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. sodium bicarbonate.
This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), epinephrine ( SGEM#238 ) and IO vs IV (SGEM#231 and SGEM#340).
Yet at the same time, despite a large-scale Holmberg study involving over 6,000 patients suggesting potential harm, epinephrine remained part of the pediatric symptomatic bradycardia protocol. That study went to the graveyard and will likely never be repeated.
” If the patient has compromise to airway, breathing or circulation, they should get immediate epinephrine. In anaphylaxis, think, “If A, B or C, give E.” D-dimer can effectively rule out a larger portion of low risk patients if age adjustment or the YEARS criteria are employed.
As part of their protocol, they attempt vascular access to administer epinephrine and an antidysrhythmic. EMS arrives on scene and initiates high quality basic life support (BLS). One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content