This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Consider these medications if there are signs of end-organ dysfunction, there is a considerable delta in baseline BP, systolic is less than 90 and/or MAP is less than 65 Norepinephrine is a good pressor for a lot of the situations that we encounter in the emergency department, such as septic shock, undifferentiated shock and hypovolemic shock.
Both norepinephrine and epinephrine can be used. Epinephrine is key if there is significant bradycardia. Spinal shock is a phenomenon of transient, physiologic (rather than anatomic) complete loss of spinal cord function inferior to an injury. Refers to the Spinal Cord Function and Reflexes, not specifically hemodynamic issues.
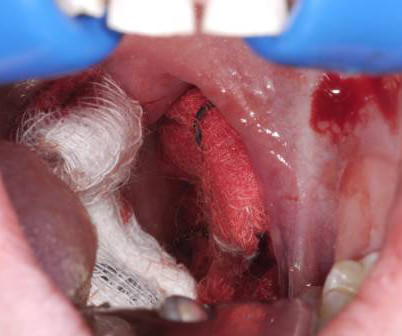
6 Apply direct pressure to the bleeding site with gauze soaked in TXA and epinephrine as a first-line intervention. 7 Epinephrine acts as a local vasoconstrictor, aiding hemostasis, and TXA helps to stabilize clot formation on the exposed tissue and delay hemorrhage progression. Its going to take time to get her to a tertiary center.
to 0.5mg (1mg/mL) IV Bolus: 5 to 20mcg (10mcg/mL) IV Infusion: 1 to 20mcg/min If Poor Response to Conventional Therapy Consider Epinephrine 100mcg IV bolus Norepinephrine infusion 0.1mcg/kg/min Vasopressin 0.01
You and your partner initiate high-quality CPR, place a supraglottic airway, establish intra-osseous (IO) access and administer epinephrine. Your partner asks if you want to administer naloxone as well. Background: We’ve discussed out-of-hospital cardiac arrest (OHCA) at least once or twice on the SGEM (see long list at end of blog).
How Long Should We Monitor After Giving IM Epinephrine for Anaphylaxis? Bottom Line Up Top: After prompt recognition and appropriate treatment with IM epinephrine, the risk of biphasic reactions are exceedingly low. At the time of discharge, appropriate patient education and prescriptions for IM epinephrine are essential.
For a full list of check out the links below to the SGEM blogs: * SGEM#50: Under Pressure Journal Club: Vasopressin, Steroids and Epinephrine in Cardiac Arrest * SGEM#54: Baby It’s Cold Outside: Pre-hospital Therapeutic Hypothermia in Out of Hospital Cardiac Arrest * SGEM#59: Can I Get a Witness: Family Members Present During CPR * SGEM#64: Classic (..)
This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), epinephrine ( SGEM#238 ) and IO vs IV (SGEM#231 and SGEM#340). first appeared on The Skeptics Guide to Emergency Medicine.
Soak the gauze with epinephrine (1:10,000) or TXA (our THIRD route of administration) Apply pressure laterally to the tonsillar fossa with the gauze covered Magill forceps. Your support staff…depending on the amount of bleeding, you are about to have your hands full and may need IV access, medications, airway management, etc. Get IV access!
A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. A Randomized Trial of Epinephrine in Out-of-Hospital Cardiac Arrest. An oral airway is placed, peripheral intravenous (IV) line started successfully and the paramedic asks her partner if you want to administer IV epinephrine? He is unsuccessfully shocked.
Intraosseous access is quickly obtained, and a dose of epinephrine is provided. Disclaimer: “While I am proud to be attending this institution, my opinions expressed here are mine alone and do not represent my residency program, hospitals I work at, or any other affiliated organizations.” ” Reference: Vallentin et al.
2 Standard management for VT and VF involves the use of electrical defibrillation, high-quality chest compressions, and epinephrine. 5 More recent literature defines “refractory” as VT or VF that is persistent or recurrent despite three shocks from a defibrillator, three rounds of epinephrine, and use of an antiarrhythmic (i.e.,
1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine.
This includes epinephrine for OHCA, target temperature management, mechanical CPR, supraglottic airways, steroids, hands on defibrillation and many more topics. Background: We have covered Out of Hospital Cardiac Arrests (OHCAs) many, many times on the SGEM.
1: Epinephrine or Airway First in OHCA? Spoon Feed In adults presenting to EMS after OHCA, those receiving epinephrine prior to advanced airway management (AAM = supraglottic airway, SGA, or endotracheal tube) experienced better outcomes and prehospital ROSC than those receiving AAM before epinephrine. JAMA Netw Open.
Vasopressor medications during cardiac arrest We recommend that epinephrine be administered for patients in cardiac arrest. It is reasonable to administer epinephrine 1 mg every 3 to 5 minutes for cardiac arrest. High-dose epinephrine is not recommended for routine use in cardiac arrest. COR 1, LOE B-R. COR 2a, LOE B-R.
After 1 mg of epinephrine they achieved ROSC. Total prehospital meds were epinephrine 1 mg x 3, amiodarone 300 mg and 100 mL of 8.4% EMS arrived and found him in Ventricular Fibrillation (VF). He was defibrillated into VT. He then underwent dual sequential defibrillation into asystole. sodium bicarbonate. Then assume there is ACS.
An inciting event will typically push them over the edge into BRASH syndrome: Dehydration Hypotension from sepsis or another condition GI illness Dosage increase of a chronic medication (e.g., beta blocker) New medication (e.g., NSAID or potassium sparing diuretic) Ask the following: Is there mild hyperkalemia? Is there some renal injury?
Written by: Sadakat Chowdhury MD Edited by: Mak Sarich MD, Jay Lin MD, Jonathan Kobles MD Background: Ultrasound (US) guided nerve blocks offer an applicable option for achieving analgesia in the emergency department. 1 2 3 4 This article will focus on three lower extremity (LE) nerve blocks commonly used for acute lower extremity pain in the ED.
Epinephrine is provided and you quickly place an advanced airway. A second dose of epinephrine is given, and you start to think about reversible causes and your next steps for in-hospital cardiac arrests (IHCA). Cardiopulmonary resuscitation (CPR) is in progress. The monitor shows a non-shockable rhythm.
Most emergency drugs except for amiodarone and succinylcholine are based on ideal body weight [Emergency Medical Services for Children, Luten 2007] Epinephrine, dopamine, fentanyl, ketamine based on what child should weigh. Reduces dosing errors during resus, up to 33.88%. Recommended by ATLS and PALS. Validation study done in Italy.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
” If the patient has compromise to airway, breathing or circulation, they should get immediate epinephrine. In anaphylaxis, think, “If A, B or C, give E.” D-dimer can effectively rule out a larger portion of low risk patients if age adjustment or the YEARS criteria are employed.
Read the 2024 ESO EMS Index Read the 2024 ESO Fire Service Index Post-Resuscitation Epinephrine Vs. Norepinephrine in Cardiac Arrest Released in May 2024 Epinephrine and norepinephrine are both commonly used as prehospital vasopressors in the United States. Missed Wave 2024 or want to revisit the highlights?
As part of their protocol, they attempt vascular access to administer epinephrine and an antidysrhythmic. One defibrillation for ventricular fibrillation (VF) is provided but the patient remains in VF. They wonder whether it would be better to attempt a peripheral intravenous (IV) line or intraosseous access first?
Myth #1: The use of non-selective NSAIDs will cause a nonunion in long bone fractures When bones break, they usually heal with either surgical or non-surgical management. Sometimes the healing process can take longer than usual (delayed union), does not heal (non-union) or in poor alignment (malunion). J Bone Joint Surg Am.
This has included things like therapeutic hypothermia ( SGEM#54 , SGEM#82 , SGEM#183 and SGEM#275 ), supraglottic devices ( SGEM#247 ), crowd sourcing CPR ( SGEM#143 and SGEM#306 ), and epinephrine ( SGEM#238 ). One aspect we have not looked at is the “load and go” vs. “stay and play” approach for OHCA.
There have been a number of papers published since OPALS that support the findings of not using ACLS drugs like epinephrine for OHCA: * Olavseengen et al. He is also the CME editor for Academic Emergency Medicine and the associate editor for emergency medicine simulation at the AAEM MedEdPORTAL. vs. 66.8%, p=0.73). JAMA 2009 * Jacobs et al.
epinephrine, histamine blockers, corticosteroids) the underlying mechanism of action predicts that these medications will not work. Though they are relatively safe, upper airway angioedema is one of the life-threatening adverse effects that we see frequently in the Emergency Department. Reference: Sinert et al.
1] The SGEM has covered the use of epinephrine, vasopressin, methylprednisolone, and calcium for cardiac arrest in SGEM#238 , SGEM#350 , and SGEM#353. . * Background: We often manage patients in cardiac arrest in the ED or the intensive care unit (ICU). But it’s not that straightforward.
In cardiac arrest, a delay in IV access subsequently results in a delay in epinephrine administration. Over the years emergency and critical care physicians have tried many ways to establish IV access in emergencies including the “crash” or “dirty” central line.
of people who take NSAIDs ( Nzeako 2010 ). patients that take ACE inhibitors (but 20-30% of all angioedema presentations to the Emergency Department) 3 times more common in Black Americans ( Kostis 2005 ) 0.01 of people who take NSAIDs ( Nzeako 2010 ). Typically involves the mouth, larynx, pharynx, and subglottic tissue ( Kostis 2005 ).
Four Critical Care Controversies: * Round#1: Mechanical CPR – SGEM#136 * Round#2: Epinephrine in Out-of-Hospital Cardiac Arrest (OHCA) – SGEM#238 * Round#3: Stroke Ambulances with CT Scanners * Round#4: Bougie for First Pass Intubation – SGEM#271 Conclusion/Winner – Use EBM and the winner is the patient We appreciate Dr.
Over the next 10 minutes we resuscitated with high doses of Calcium, Epinephrine, and Bicarbonate. There was no IV access, so we obtained intraosseous (IO) access, but she arrested before we could give her all the calcium. Weakness and Dyspnea with a Sine Wave. It's not what you think! A Very Wide Complex
1,2] Consider using a physiological marker to help identify inadvertent vascular injection, such as epinephrine. [3] 1,2] Consider using a physiological marker to help identify inadvertent vascular injection, such as epinephrine. [3] If epinephrine is used, small initial doses ( <1 ug/kg) are preferred. mL/kg/min. [2]
Be aggressive with fluid resuscitation and consider epinephrine up to 0.06–0.08 Audio quality was a bit dodgy in this one; sorry all!–eds.] Most routine cases will aim to be “bloodless,” i.e. only transfusing autologous (“Cell Saver” blood), as transfusion of banked blood is considered an STS measure.* vancomycin).
Disease-Oriented Outcomes (DOOs) The PARAMEDIC-2 trial looked at the effectiveness of epinephrine in adult patients who suffered an out-of-hospital cardiac arrest. They found that epinephrine administration was associated with higher survival at 30 days ( 3.2% A randomized trial of epinephrine in out-of-hospital cardiac arrest.
Epinephrine at lower doses is a good second line, providing inotropic support for the RV without much impact on PVR. Takeaway lessons * Evaluate for the risk of decompensation in a patient with known PH and acute illness by considering their most recent echocardiogram, and repeating it as soon as possible after admission.
They continue CPR, get intravenous access, give a round of epinephrine and then wonder if they should start rapid cooling en-route to the hospital with some cold saline. By-standard CPR is started and EMS is called. They arrive quickly and take over the resuscitation. She is not in a shockable rhythm.
Check the pulse RSI= Resuscitation Sequence Intubation Hypoxia, Hypotension, and Acidosis are the reason patients code during/post intubation These patients are super high risk for all 4 Optimize first pass success – Induction agent + paralytic Unconscious patients will still have muscle tone Induction Ketamine or Etomidate at half doses (i.e.,
In the ED he received methylprednisolone, diphenhydramine, and epinephrine for possible anaphylaxis. Shortly after receiving epinephrine, the patient developed new leg cramps and chest pain. The chest pain was described as sharp and radiated to both arms. A "STEMI alert" was called and soon cancelled.
Traditional Advanced Cardiovascular Life Support (ACLS) medications, namely epinephrine, have been known to exacerbate coronary vasospasm. Overall, cardiac arrest in the setting of coronary vasospasm is thought to be relatively uncommon. Cardiac arrest secondary to myocardial ischemia from coronary vasospasm is well documented.
link] __ Case continued There was hypotension, initially controlled with an epinephrine infusion. Bedside ED ultrasound showed exceedingly poor global LV function, and no B lines. Here is the initial ED ECG. What do you think? Rhythm : Residents asked me why it is not VT. So it must be atrial fibrillation.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content