This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Their hospital has struggled with a growing number of adverse events that often occur without warning. These systems use real-time data from electronic health records (EHRs) and other sources to predict which patients are at risk of adverse outcomes, such as cardiac arrest or transfer to an intensive care unit (ICU) [1.2].
He is board certified […] The post SGEM#368: Just A Normal Saline Day in the ICU – The PLUS Study first appeared on The Skeptics Guide to Emergency Medicine. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates. .
We discuss the field of rehabilitation psychology, and how it can help patients with persistent critical illness, with Dr. Megan Hosey (@DrMeganHoseyPhD), clinical psychologist and assistant professor at Johns Hopkins School of Medicine, where she practices in the medical ICU. Delirium often dominates the patient experience of the ICU.
He is also director of their Outcomes After Critical Illness … Continue reading "Episode 26: ICU sedation, mobility, and delirium with Dale Needham" How to manage the intubated critically ill patient while keeping them awake, non-delirious, and mobile, with Dr. Dale Needham, FCPA, MD, PhD. .*
PMID: 37611862 Clinical Question: In patients treated in the ICU, can a protocol of peripheral IV catheter vasopressors safely reduce the number of days of CVC use and frequency of placement? No Extravasation Event vs Extravasation Event Age: 63 vs 67 years BMI: 28.3 Not met in 15.7% All Catheter Criteria Met: 44.3%
Mild to moderate DKA represents a subgroup of patients that often require admission to the ICU due to hospital policies not allowing insulin infusions outside of this clinical setting. to 19.3hrs); Reduction by 3.6hrs ED LOS was shorter for the SQuID cohort ICU Admissions: SQuID & Traditional (Post Intervention): 42.9%
The idea behind abx is to prevent things like AOM and TSS but neither should be much of an issue with short term placement ICU Admission? Traditional teaching is that these patients are at risk for life-threatening bradydysrhythmias and should go to the ICU Literature here is non-existent. Acad Emerg Med 1995; 25(5): 592-6.
That discussion can be deferred until the patient is stable, the risk of such an event is mitigated, and other medications can be given for their withdrawal symptoms and pain. Multi-Substance Use Substances such as cocaine, amphetamines, and benzodiazepines often are used concurrently, which can confound the management plan.
How to take the well-resuscitated critically ill patient, get fluid out of them, deescalate their antibiotics, wean their sedation, reduce vent support, extubate, and get them out of the ICU—with Dr. Matt Siuba (Twitter: @msiuba), an intensivist at the Cleveland Clinic with an abiding interest in “zentensivism,” the art of doing less.
From a safety standpoint this is a great thing, but also could be the reason we see such few adverse events Discussion: There is a recent “push” to utilize “Push dose pressors” as the correction of acute hypotension in a variety of clinical scenarios. In other words these were pre-made syringes and not mixed at the bedside. Am J Emerg Med.
Hospital Events: With 8% of patient encounters involving at least one hospital event, such as unexpected ICU admissions or delirium, the Index identifies a significant area to reduce for improvement in patient safety and care quality.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Population: Adult patients ( > 18 years of age) admitted to the ICU with COVID-19 and severe hypoxemia (defined as receiving supplemental O2 with a flow rate of at least 10L/min or receiving mechanical ventilation or non-invasive ventilation. 0.83 (0.66 – 1.13) NO Adverse Events 51.7% days (0.2 – 11.5)
A 65 y/o Female was admitted to the ICU for septic shock. Beats 9-12 : Continuation of the previously described events, all inducible by the pause (and thus, prolongation of refractoriness) created by the PVC of Beat 8. She was critically ill despite aggressive vasopressor therapy.
Background:Patients diagnosed with COVID-19 have an increased risk of thromboembolic events, including pulmonary embolism and deep vein thrombosis (DVT). The INSPIRATION Trial investigated outcomes with an intermediate vs. standard prophylactic dose of anticoagulation in ICU patients.
Diurese until you develop flow problems (suction events) on the pump, a useful indicator of low intravascular volume.* Decannulate at the bedside when ready, watch them for 24 hours, then boot them out of the ICU; they’re ready.* Inhaled vasodilators can be continued or weaned depending on right heart function.
ICU: 42.6% 4.70) in grade 2-4 bleeding event Subgroup analysis revealed a higher risk of grade 2-4 bleeding was noted with decreasing platelet counts, and the greatest benefit of platelet transfusion is likely to be in those patients with a lower platelet count. ICU: 42.6% ICU Mortality: 56.7% ICU Mortality: 56.7%
Background: Severely ill patients diagnosed with COVID-19 have an increased risk of cardiovascular complications, especially thromboembolic events (Bikdeli 2020). Multiple studies have investigated the use of antithrombotic agents in patients with COVID-19 admitted to various hospital settings (Talasaz 2021).
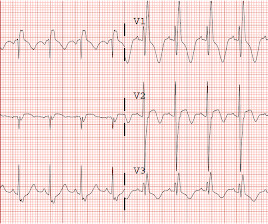
The patient was admitted to the ICU. The potassium was repleted in the ICU to a total of 170 mEq with resolution of symptoms (this could be hazardous!). mEq/L on discharge without telemetry events. Large U-waves confirm the diagnosis of hypokalemic periodic paralysis (HPP). The K returned at 1.4 mEq/L and K was given po and IV.
Study Overview A recent research study titled “Sodium Bicarbonate Use During Pediatric Cardiopulmonary Resuscitation: A Secondary Analysis of the ICU-RESUScitation Project Trial” aimed to evaluate the associations between sodium bicarbonate use and outcomes during p-IHCA. 1.34; p = 0.621).
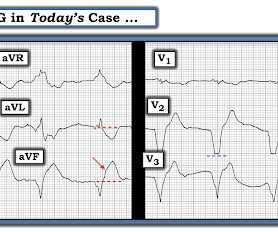
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. KEY Point: The important distinction that has to be made in today's case, is between ECG findings consistent with this patient's prior LAD OMI — vs — ECG findings of a new acute event superimposed on these prior ECG findings.
While not specifically reviewed in this post, check out the methemoglobinemia tox card for more information about one of the other known events that can occur with local anesthetic administration. Hemodynamics slowly begin to stabilize, and the patient is transferred to the ICU for further post-cardiac arrest care.
The group that received phenobarbital had a higher maximum CIWA score than the group that received lorazepam, which could mean that phenobarbital was not as effective as lorazepam, although this is potentially confounded by patients who were transferred to the ICU were excluded from the study.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Course : A CT of the head, neck, chest, abdomen and pelvis showed no other unanticipated injuries and she was admitted to the ICU. Patients may have positive biomarkers (troponin) from the related stress of multisystem trauma, and low levels of troponin probably do not predict adverse events any better than the patients clinical condition.
The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. Once a sufficiently high level is achieved, modelling of behaviours and episodes of retaliation can perpetuate the behaviours far beyond the initial event. How do you manage this situation?
TTP is a lovely ICU diagnosis. TTP is a lovely ICU diagnosis. Welcome back to the tasty morsels of critical care podcast. Not so much for the patient but it’s one of those ones that is niche enough to not have been picked up via the. Read More » Welcome back to the tasty morsels of critical care podcast.
Given that a lot of ICU bed days are given over to managing SAH, I felt it might have warranted its own chapter. Hydrocephalus is a relatively common event in SAH and the theory is that blood in the CSF space blocks up the arachnoid granulations preventing reabsorption and with ongoing production and failure to reabsorb you get hydrocephalus.
Candidiasis is common in ICU patients. That being said knowing what’s there in the event of the patient getting super sick might be somewhat helpful in guiding therapy. These are work horses in the ICU with a low side effect profile and importantly cover the vast majority of candida likely to grow.
Neurology consultation should be initiated, and the patient should be admitted to the ICU. Alternatively, the Neurocritical Care Society defines it as a seizure with five minutes or more of continuous clinical or EEG seizure activity, or recurrent seizure activity without recovery between seizures.
We have already converted pediatric hospitals to accept adult patients, our backup docs are working full schedules, our nurses are working double time, the ED functions as an additional ICU, and we are stretched to our limits with no end in sight. The emotional toll that this is waging on many of us is very concerning.
Peak levels occur ~15-120 mins post event and decline predictably (T1/2 ~2hrs). Oh is quite pro IV infusions and certainly in the ICU and OT this is ubiquitous and generally well done in my experience.
He went into cardiogenic shock and is intubated in the cardiac ICU. The main premise of my qualitative approach — is to be suspicious of an acute cardiac event when you see ST-T wave findings that shouldn't be there. I just got the follow up that he had a near complete very proximal LAD occlusion , and a complete PDA occlusion.
Wellens' is a syndrome of a painless period following an anginal (chest pain) event. She had an uneventful ICU course and improved steadily over the course of a week. Thus, it is critical to compare the ECG with the symptomatic state of the patient! Differences of Pulmonary Embolism T-waves from Wellens' T-waves: 1.
The patient was managed in the ICU and had serial troponins. (THE PM CARDIO OMI AI APP) If you want this bot to help you make the early diagnosis of OMI and save your patient and his/her myocardium, you can sign up to get an early beta version of the bot here. It is not yet available, but this is your way to get on the list. First was 2.9
Effectiveness of Nasal High-Flow Oxygen during apnoea on Hypoxaemia and Intubation Success in Paediatric Emergency and ICU Settings: a randomised, controlled, open-label trial. Thats exactly what Shane George et al. George S, Williams T, Humphreys S, et al. Lancet Respiratory Medicine. Hypoxaemia occurred in 12.8% in the standard care group.
I found a well appearing young lady in the room with her parents who witnessed the event. She denied having any symptoms before or after the event, and she was asymptomatic on my initial exam. She was diagnosed with pericarditis and spent one day in the hospital without events.
3, 4 It is the most common nosocomial infection in patients on mechanical ventilation, and one of the leading causes of nosocomial infection among all patients in the ICU. To confirm VAP, events were defined in a standardized approach using the American Thoracic Society criteria. 4, 8 Paper: Dahyot-Fizelier, C.,
PMID: 38019968 Clinical Question: In patients with suspected acute poisoning and GCS <9, is a conservative airway strategy of withholding intubation associated with a reduction in death, ICU LOS, and hospital LOS compared with routine practice of intubation? References: Freund Y et al.
They consecutively enrolled 1,817 ICU patients from 45 sites across China. Population: Inclusion Criteria: Age 18-75 years old SOFA score 2-13 Admitted to the ICU with a diagnosis of sepsis 3.0, “ Life-threatening organ dysfunction caused by a dysregulated host response to infection.” 002) ICU-free days: Placebo 12.4%
This could potentially help improve thrombin generation, reduce blood product consumption, but also could increase the risk of thromboembolic events. Additionally, the use of 4F-PCC resulted in a higher rate of thromboembolic events compared to placebo. 4F-PCC contains factors II, VII, IX, X as well as Proteins S and C.
What They Did: Single-center, parallel, double blind, randomized controlled trial performed in a medical-surgical ICU (Mexico) Both groups received: Adjunctive vasopressin initiated at a dose of 0.03 It also reduced length of stay in ICU and hospital without adverse effects. NaCl over 6hrs once daily x3 doses Placebo: 500mL of 0.9%
Disposition to ICU. Potassium Shifted intracellularly by insulin, total body potassium is normal Replete to goal 3-3.5 Reinforces importance of close monitoring and intervention. Takes 30 minutes to see effect, temporize with traditional vasopressors (norepinephrine, vasopressin). References: Yuan TH, Kerns WP, Tomaszewski CA, et al.
Given the presentation, the cardiologist stented the vessel and the patient returned to the ICU for ongoing critical care. (TIMI 3 means the rate of passage of dye through the coronary artery is normal by angiography.) Lesions less than 70% are generally considered to be non-flow limiting. Two subsequent troponins were down trending.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content