This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These systems use real-time data from electronic health records (EHRs) and other sources to predict which patients are at risk of adverse outcomes, such as cardiac arrest or transfer to an intensive care unit (ICU) [1.2]. Despite the potential benefits, integrating AI into clinical workflows presents challenges.
A roundup from members of the SCCMs ICU Liberation committee, recorded at SCCM Congress 2025. Included: A roundup from members of the SCCM’s ICU Liberation committee, recorded at SCCM Congress 2025.
Caleb Lin Hyperbaric Oxygen for the ICU Patient OVERVIEW INTENSIVE CARE INDICATIONS PRACTICAL ISSUES IN CRITICAL CARE Consideration & Prior to Treatment In the Chamber A: ETT cuff to be filled with sterile water or connected to dynamic cuff inflator B: Titrate ventilation to PaCO2, note that EtCO2 is not linearly proportionate at higher pressures (..)
Fever in the Emergency Department Predicts Survival of Patients With Severe Sepsis and Septic Shock Admitted to the ICU. Outside his family and work, Jesse pours […] The post SGEM#195: Some Like It Hot – ED Temperature and ICU Survival first appeared on The Skeptics Guide to Emergency Medicine. Critical Care Medicine 2017.
Today we'll walk through some interesting bits of the new IDSA/SCCM guideline on evaluation of new fever in the adult ICU patient (available free here). More guidelines! how should temperature be evaluated? This is frankly a mess. Bladder catheter or esophageal probe are best, but usually not used.
He is board certified […] The post SGEM#368: Just A Normal Saline Day in the ICU – The PLUS Study first appeared on The Skeptics Guide to Emergency Medicine. Exclusions: Patients with specific ICU fluid requirements, those who received disqualifying fluid prior to enrollment (> 500 mL in the ICU),
Discussing ICU triage, risk stratification, and patient disposition with intensivist Eddy Joe Gutierrez (@eddyjoemd) of the Saving Lives Podcast. Takeaway lessons * When a patient has borderline indications for requiring the ICU, generally, in the real world, they should go to the ICU. When a sending provider (e.g.
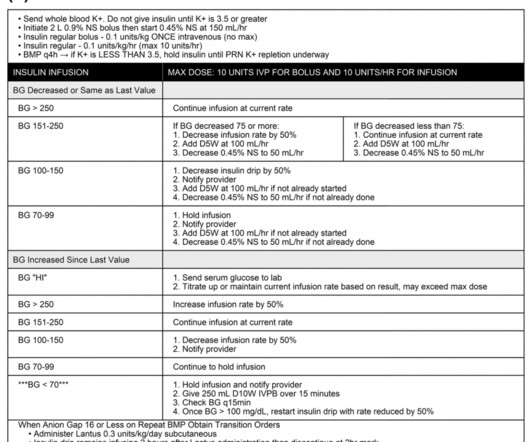
The standard of care of treating DKA is fluid resuscitation, electrolyte management, and intravenous insulin infusion in the intensive care unit (ICU) setting for close glucose and electrolyte monitoring. Recent research aims at investigating the treatment of DKA with subcutaneous insulin in non-ICU settings. Image from cited article.
The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” However, the ICU is full and the patient will likely be boarding in your ED for a bit before coming upstairs.
We discuss the practical barriers to implementing the A-F ICU liberation bundle, with Kali Dayton, ACNP-BC (@HomeIcu), host of the Walking Home from the ICU podcast, and consultant to ICUs working on these issues. Learn more at the Intensive Care Academy! Find us on Patreon here! Buy your merch here! Find us on Patreon here!
Bryan and Brandon talk about the physical exam: how we apply it in the ICU, its utility and changing role in the setting of modern diagnostic modalities, and its best and most practical use-cases. References McNamara LC, Kanjee Z. Counterpoint: Routine Daily Physical Exams Add Value for the Hospitalist and Patient. J Hosp Med. J Hosp Med.
To claim your CME … Continue reading "Episode 52: Pleural effusions in the ICU with Emily Fridenmaker" Discussing pleural effusions in the critically ill, including how and when to drain them, methods of drainage, interpreting laboratory studies, and managing complications, with Dr.
Brandon and Bryan talk about the practicalities of communication, collaboration, and compromise in a surgical ICU, when the surgical and critical care teams are both involved, one is the “primary” team on paper, but everyone needs to be heard.
However, it also causes a variety of unique and severe side-effects, which frequently cause ICU admission. CAR-T cell therapy is rapidly expanding as a miraculous therapy for numerous malignancies.
He is also director of their Outcomes After Critical Illness … Continue reading "Episode 26: ICU sedation, mobility, and delirium with Dale Needham" How to manage the intubated critically ill patient while keeping them awake, non-delirious, and mobile, with Dr. Dale Needham, FCPA, MD, PhD.
James Pearlman Introduction to an ICU rotation Introduction to an ICU rotation. This page is intended as an introduction to ICU core topics why the author enjoys Intensive Care Medicine
All of the secondary outcomes (mortality at 90 days, misdiagnoses, hospital length of stay, ICU admission rate, ICU length of stay, and quality of life) also did not show a statistical difference between the intervention group and the control group (SGEM#207).
We discuss the field of rehabilitation psychology, and how it can help patients with persistent critical illness, with Dr. Megan Hosey (@DrMeganHoseyPhD), clinical psychologist and assistant professor at Johns Hopkins School of Medicine, where she practices in the medical ICU. Delirium often dominates the patient experience of the ICU.
Supportive Care Intensive monitoring, often in an ICU setting. Adjunct Therapies Hyperbaric Oxygen Therapy (if available) for resistant cases. Evidence is mixed; not universally accessible. Fluid resuscitation & vasopressors for septic shock.
Date: April 25, 2024 Guest Skeptic: Missy Carter is a PA working in an ICU in the Tacoma area and an adjunct faculty member with the Tacoma Community College paramedic program. Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation.
Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. With both ER and ICU experience, this post acts as a quick […] The post Mechanical Ventilation Basics appeared first on EMOttawa Blog.
We chat with Noelia Bischoff, recently off orientation in the medical ICU at Johns Hopkins as a nurse practitioner, about the transition from her role as a bedside ICU nurse. Check out the Intensive Care Academy here! Find us on Patreon here! Buy your merch here! Check out the Intensive Care Academy here! Find us on Patreon here!
Polypharmacy is technically defined as taking five or more medications on a daily basis. Polypharmacy is increasingly becoming the norm among adults, due to several factors (an aging population, increasing numbers of medical problems, and increasingly complex regimens available to treat chronic disorders such as heart failure).
Resources * ICU Liberation.org * ICU Delirium * ICU Rehab Network Resources A roundup of opinions from attendees at SCCM’s 2024 Critical Care Congress in Phoenix on strategies for rescuing the patient stuck in a loop of deep sedation and agitation.
Historically, it has been used more frequently in the ICU than in Emergency Departments, likely due to provider comfort. […] The post Is there a Precedence for Precedex in the ED? It offers a unique profile of sedation without respiratory depression, making it an attractive option in various clinical scenarios.
This is based, in large part, on indirect evidence illustrating the benefits of adjunctive phenobarbital including, but not limited to, reduction on the need for intubation, decreased hospital length of stay, decreased ICU admission and length of stay.
An overview of the role and contributions of a clinical pharmacist in the ICU, with Laura Means Ebbitt of the University of Kentucky, a clinical pharmacist specializing in colorectal/ENT surgery and critical care. Takeaway lessons A clinical pharmacist is a “knowledge pharmacist,” dispensing advice rather than medications.
Consequently, a single person will often be responsible for both inpatient ICU management as well as inpatient pulmonary consultation. In many countries, pulmonary and critical care are commonly bundled together. Honestly, I have some doubts about whether this is an ideal system.
Several studies have indicated that dosing with phenobarbital (PO or IV) is safe and effective at decreasing the need for escalating doses of benzodiazepines for EtOH withdrawal [1-6].
Leon is an Adult/Gerontology Acute Care Nurse Practitioner in the ICU, Clinical Program Manager of Research and Simulated Learning, and an Associate Professor at Columbia University School of Nursing. We chat with Leon Chen about his work setting up infrastructure for clinical POCUS at Memorial Sloan Kettering. Find us on Patreon here!
It is unacceptable to have the rates of Awareness during Paralysis seen in a recent ED sedation study--We are better than this. EMCrit Project by Scott Weingart, MD FCCM.
I would view this as the triquel following SUP-ICU and PEPTIC. In order to understand REVISE in context, let's briefly review SUP-ICU and PEPTIC trials, before discussing REVISE. Part I: SUP-ICU (2018) This was a large multicenter RCT […] EMCrit Project by Josh Farkas.
Stress hyperglycemia is an everyday occurence in the ICU, but we hardly know how to treat it. (Blogitorials are short, informal blogs that are written in the spirit of a tweetorial). I've been waiting years for this topic to be clarified… but I've realized that such clarity will probably never be reached.
PMID: 35387313 Clinical Question: Do prehospital antibiotics impact 28 day mortality, length of stay in the hospital and ICU length of stay for patients triggering sepsis compared to usual care (No prehospital antibiotics)? to 0.97; p = 0.02 to 2.07; p = 0.91 to 12.33; p = 0.26 to 0.97; p = 0.02 to 2.07; p = 0.91 to 12.33; p = 0.26
Our residents are currently the primary staff members in our Shoreline emergency department, had of the medical ICU, and the entire Trauma ICU. “We feel that this decision was made without adequate assessment of the negative impacts this WILL have on our patients.
A recent prospective study was published in CHEST regarding the use of peripheral administration of Norepinephrine in ICU. 603 patients received medication through peripheral IV access, and they found almost half of patients did not require central access, and 35 patients had extravasation with no significant complications. Link to article
The use of direct oral challenges has been tried in the intensive care unit (ICU) setting to de-label patients. Koo et al showed that offering amoxicillin oral challenges to ICU patients with low-risk penicillin allergies.
So, from the ultra broad topic of AKI in the last podcast to the super specific question of when we should pursue an open lung biopsy in an ICU patient. So, from the ultra broad topic of AKI in the last podcast to the super specific question of when we should pursue an open lung biopsy in an ICU patient.
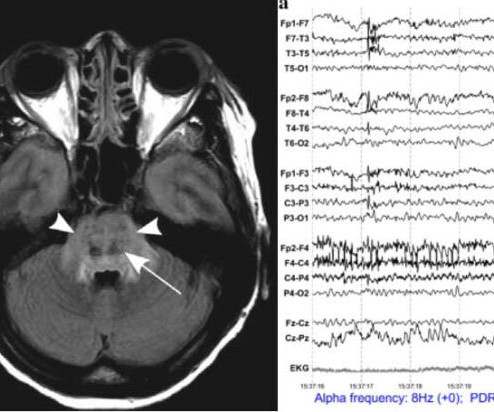
Management of the a patient following craniotomy focuses on the fundamentals of supportive neurocritical care. However, special attention is required to unique postoperative complications that may occur (depending on the procedure). The IBCC chapter is located 👉 here. The podcast & comments are below. Follow us on iTunes.
Time is always a factor in the ICU, but some time matters more than other time. Time is always a factor in the ICU, but some time matters more than other time.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content