This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
GRACE1: Recurrent, Low-Risk Chest Pain GRACE2: Recurrent, Low-Risk Abdominal Pain GRACE3: Acute Dizziness & Vertigo For this SGEMHOP Xtra combo episode on GRACE4, we are going to give a case scenario, a little background information, ask a clinical question, provide authors’ conclusions, go through the recommendations and a case resolution.
Clinical impact: Rather than arguing with the patient about the likelihood of this phenomenon occurring and whether this is a true allergy, the patient is informed that they do not need to immediately start treatment to receive care in the hospital. The Necessity of a Trauma-Informed Paradigm in Substance Use Disorder Services.
(Blogitorials are short, informal blogs that are written in the spirit of a tweetorial). Stress hyperglycemia is an everyday occurence in the ICU, but we hardly know how to treat it. I've been waiting years for this topic to be clarified… but I've realized that such clarity will probably never be reached.
Author information T. Several studies have indicated that dosing with phenobarbital (PO or IV) is safe and effective at decreasing the need for escalating doses of benzodiazepines for EtOH withdrawal [1-6]. In: StatPearls. StatPearls Publishing; 2023. Accessed April 16, 2023. Alcohol withdrawal. EMCrit Project. Published March 29, 2023.
While community acquired pneumonia (CAP) is 'bread and butter' emergency medicine, and the diagnosis is often a 'slam dunk', it turns out that up one third of the time, we are wrong about the diagnosis; that x-rays are not perfect; that blood work is seldom helpful; that not all antibiotics are created equal and that deciding who can go home and who (..)
Our residents are currently the primary staff members in our Shoreline emergency department, had of the medical ICU, and the entire Trauma ICU. Watch the ACEP Now website for more information as it becomes available. We fear that this decision will negatively impact patient safety and quality of care.”
In shocky patients, arterial lines are often used to monitor hemodynamic parameters and inform treatment decisions. PMID: 38215002 Clinical Question: In critically ill adults in the ICU is noninvasive blood pressure (NIBP) monitoring similar (≤10% difference) to invasive arterial blood pressure (IABP) monitoring? to 1.12; p = 0.03
In our emergency department, the RTs do not spend a lot of time going around measuring cuff pressures and usually save that until the patient reaches the ICU. Hence, the RT’s are supposed to have them. It is convenient to use for the inflation of the esophageal balloon because it can inflate and measure pressure at the same time.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
How to take the well-resuscitated critically ill patient, get fluid out of them, deescalate their antibiotics, wean their sedation, reduce vent support, extubate, and get them out of the ICU—with Dr. Matt Siuba (Twitter: @msiuba), an intensivist at the Cleveland Clinic with an abiding interest in “zentensivism,” the art of doing less.
It does this by doing a structured critical review of a recent publication and then disseminates the information using the power of social media. The SGEM strives to make the information accessible with the right balance of education and entertainment. We want patients to get the best care based on the best evidence.
A retrospective look at aggregate data, the purpose of the following metrics is to both inform and ignite a conversation around best practices to help improve patient outcomes. To decide what metrics would be most helpful to include, ESO data scientists reviewed medical journals throughout the year, taking note of hot-button topics.
Background Information: Obtaining definitive control of the airway, when indicated, is the responsibility of the emergency medicine physician. 2 Finally the settings initiated early in a patient’s care are often carried forward unchanged into their hospital and ICU stay. Paper: Owyang CG, et al. J Crit Care.
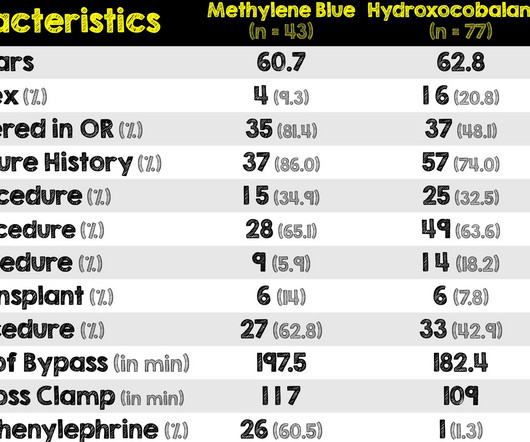
Background Information: Vasoplegic shock is defined as hypotension with normal or increased cardiac output and can commonly occur in post-cardiac surgery patients having received cardiopulmonary bypass. This dysregulation of vasodilation is associated with a mortality of close to 25%.
PMID: Clinical Question: Does a single dose of ketamine or etomidate used for rapid sequence intubation (RSI) of critically adults in the ED impact the SOFA score within 3 days of hospitalization? Range 5 to 9) Etomidate: 7.0 Range 5 to 9) Diff -0.2; 95% CI -1.4
Background Information: Acute Hypotension is associated with increased morbidity and mortality. The retrospective design of this study omitted assessment of ventricular dysrhythmias related to push dose pressor administration, as they were reliant on information in the EMR. J Med Toxicol. Epub 2019 Jul 3. Intensive Care Med.
Background information : Alcohol has potentiating effects on the inhibitory GABA neurotransmission system and inhibitory effects on the excitatory glutamate neurotransmission system. Limitations : More information would have been helpful regarding the statistical methods regarding propensity scores.
We discuss the basics of EEG in the ICU, including when to do it, selecting the appropriate study, and the basics of bedside interpretation, with Carolina B Maciel, MD, MSCR, FAAN, triple boarded in neurology, neurocritical care, and critical care EEG. Learn more at the Intensive Care Academy! Find us on Patreon here! Find us on Patreon here!
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
As such it presents a fairly predictable work load and patient cohort for your ICU. Given the bewildering number of conditions that can present to a mixed ICU on a given day, knowing that you have a couple of hearts moving along the production line provides a degree of predictability to the workflow.
ICU: 42.6% vs 0% ICU length-of-stay: 9 days vs 7 days In-Hospital Mortality: 28.2% ICU Mortality: 56.7% Conversely, it may be reasonable to withhold prophylactic platelets for patients in the ICU setting due to trends of lower bleeding risk noted as well as more intensive bleeding monitoring. Median hemoglobin: 8.2
While not specifically reviewed in this post, check out the methemoglobinemia tox card for more information about one of the other known events that can occur with local anesthetic administration. Hemodynamics slowly begin to stabilize, and the patient is transferred to the ICU for further post-cardiac arrest care.
The team sits down for a hot debrief once the patient is stabilised and transferred to the ICU. Exposure impairs information sharing and overall team collaboration. While you are leading the resuscitation, one of your senior colleagues belittles a junior staff member for struggling to site an IV line. How do you manage this situation?
Hopefully in a few minutes you’ll at least have a few morsels more of information to stave off all the trainees who are undoubtedly much smarter than you on the ward round. It is important to realise that a referral to ICU for refractory cardiorenal syndrome may simply be a sign that the patient is reaching end of life.
You retrieve the below relevant information… Vital signs : T 40, HR 140, BP 75/40 (52) Examination : mucous membranes slightly dry, skin turgor normal, mild dependent pitting oedema Bloods: Na 146, K 5.2, A urinary catheter was also inserted. She has been commenced on broad-spectrum IV antibiotics. Intensive Care Med. 2018;44(4):409-417.
The main use of this information will come when some smug consultant corrects one of the team when they say PCP instead of PJP and then to rescuse the juniors from their shame you can bust out the ICNafp declaration on the two “i”s and arise victorious over said smug consultant.
Contacted authors of included studies for additional information when necessary Checked multiple trial registries for unpublished literature Included studies from multiple countries Included all ages Included all languages Investigators assessed quality with standardized critical appraisal instruments from the Joanna Briggs Institute (JBI).
Evaluate and treat seizures or SE after CA in the context of other available clinical information because other systemic factors may influence the occurrence of seizures or SE and the effectiveness of treatment (90%, 18/20). Digestive Management Takeaway: Start enteral feeds when the patient gets to the ICU. Start low and go slow.
A lot of that comes because it is a “syndrome”, ie a collection of clinical findings that someone has put into a big bucket and mixed around without paying too much attention to hard core diagnostic information like histology or a true pathological diagnosis. To start with we need context. To start with we need context.
I have accumulated a large number of summarised and truncated notes across two specialties (three if you include the echo stuff…) and they exists as a useful compilation of information that I felt tricky enough and important enough to create a note for.
The goal, of course, is to provide clinicians with faster results, automate the analyses of patient data, and help them make better informed decisions about a patient’s care. AI is already playing a major role in medical imaging by helping to automate image analysis and reduce the amount of time needed to interpret scans.
While MRI is more resource and time intensive, studies have shown that a 6-minute protocol can give sufficient information to dictate treatment in the right setting. 15 DWI MRI sequence can show an acute brainstem or cerebellar infarct within seconds of the arterial occlusion.
Background Information: Atrial fibrillation with rapid ventricular rate (RVR) is one of the many tachydysrhythmias we encounter in the Emergency Department (ED). 2 Amiodarone is commonly known for its anti-arrhythmic properties and a commonly used agent in the Intensive Care Unit (ICU).
I texted this to Dr. Smith without any information, and this was his reply: "This could be pericarditis but probably is normal variant." in the ICU but survived with excellent function. Our THANKS to Dr. Meyers for presenting this informative case! I do not believe there is any finding here suggestive of OMI.
However, this additional information was supportive. I took part in her ICU care and she was extubated and stable to transfer to a stepdown unit after a few days. Note that by current guidelines, this patient had a NSTEMI, but it would hard to argue that her condition would not have worsened if she was left to 'next day cath'.
The reality of ever increasing ED volumes and longer boarding times to the ICU makes it imperative for emergency physicians to learn how to manage these critical patients. It was found that patients exposed to deep sedation in the ED had an independent higher incidence of continued deep sedation on ICU day one ( Fuller, 2019 ).
They informed me that she had just been hospitalized 10 days ago for "some fluid around the heart" and was discharged after one day without incident. More specific information such as definitive RV diastolic collapse was not indicated or available at this time given the obvious clinical context.
Background Information: Delirium is a common and serious condition in patients in the intensive care unit (ICU). It is estimated to affect 30-50% of patients in the ICU and haloperidol is the most frequently used agent in treatment (3). Paper: Andersen-Ranberg NC,et al; AID-ICU Trial Group. N Engl J Med. 2022 Dec 29.
Effectiveness of Nasal High-Flow Oxygen during apnoea on Hypoxaemia and Intubation Success in Paediatric Emergency and ICU Settings: a randomised, controlled, open-label trial. Its pragmatic design ensured that a broad range of clinical presentations were included across the ED and ICU settings. Thats exactly what Shane George et al.
REBEL Cast Ep119: A Discussion with Scott Weingart on the CT FIRST Trial Click here for Direct Download of the Podcast Timing Is 6hrs reasonable because most pts excluded because of this Right before heading up to ICU seems good 1st couple hours after ROSC…pts are high risk for re-coding Where Not single coverage or stand-alone EDs Optimize and transfer…scans (..)
Question: In adult patients admitted to the ICU with severe CAP, does hydrocortisone compared to placebo reduce 28-day all-cause mortality? Question: In adult patients admitted to the ICU with severe CAP, does methylprednisolone compared to placebo reduce 60-day all-cause? CT can provide important information. N Engl J Med.
Secondary Outcomes: Delayed hypotension, increased ICU stay, and other relevant outcomes. It’s not mentioned whether the authors attempted to identify additional studies by checking the references of the selected articles or by contacting the original paper authors for more information. 2.89, p = 0.01.
Population: Children <18 year from Pediatric Health Information System (PHIS) database hospitalized with Influenza from 2007-2020. Association of early oseltamivir with improved outcomes in hospitalized children with influenza, 2007-2020. JAMA Pediatr.
Background Information: Acute kidney injury (AKI) is one of the most frequent complications of cardiac surgery and the cause is complex. Renal hypoperfusion from decreased glomerular filtration rate after cardiopulmonary bypass is a major contributor.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content