This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
These systems use real-time data from electronic health records (EHRs) and other sources to predict which patients are at risk of adverse outcomes, such as cardiac arrest or transfer to an intensive care unit (ICU) [1.2]. Despite the potential benefits, integrating AI into clinical workflows presents challenges.
Caleb Lin Hyperbaric Oxygen for the ICU Patient OVERVIEW INTENSIVE CARE INDICATIONS PRACTICAL ISSUES IN CRITICAL CARE Consideration & Prior to Treatment In the Chamber A: ETT cuff to be filled with sterile water or connected to dynamic cuff inflator B: Titrate ventilation to PaCO2, note that EtCO2 is not linearly proportionate at higher pressures (..)
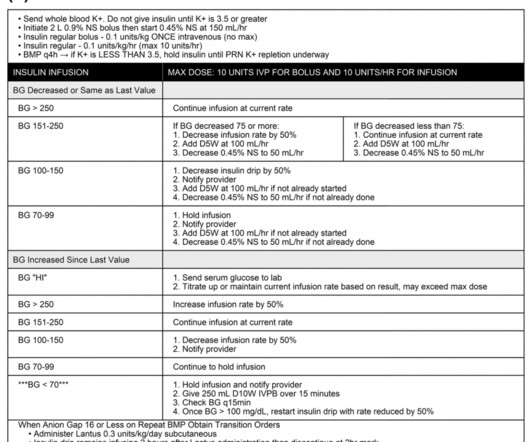
The standard of care of treating DKA is fluid resuscitation, electrolyte management, and intravenous insulin infusion in the intensive care unit (ICU) setting for close glucose and electrolyte monitoring. Recent research aims at investigating the treatment of DKA with subcutaneous insulin in non-ICU settings. Image from cited article.
The patient states he has had multiple “diabetic emergencies” in the past and usually ends up in the intensive care unit (ICU) on a drip. He is wondering, “Hey doc, do I have to go back to the ICU strapped to an IV pole?” However, the ICU is full and the patient will likely be boarding in your ED for a bit before coming upstairs.
Today we'll walk through some interesting bits of the new IDSA/SCCM guideline on evaluation of new fever in the adult ICU patient (available free here). how should temperature be evaluated? This is frankly a mess. Bladder catheter or esophageal probe are best, but usually not used.
He is board certified […] The post SGEM#368: Just A Normal Saline Day in the ICU – The PLUS Study first appeared on The Skeptics Guide to Emergency Medicine. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates.
Discussing ICU triage, risk stratification, and patient disposition with intensivist Eddy Joe Gutierrez (@eddyjoemd) of the Saving Lives Podcast. Takeaway lessons * When a patient has borderline indications for requiring the ICU, generally, in the real world, they should go to the ICU. When a sending provider (e.g.
Supportive Care Intensive monitoring, often in an ICU setting. Types of Necrotizing Fasciitis Type I (Polymicrobial) Involves aerobic and anaerobic organisms (e.g., Bacteroides, Clostridium, Peptostreptococcus). Common in immunocompromised patients or those with comorbidities (e.g., diabetes, peripheral vascular disease).
Emily Fridenmaker (@emily_fri), pulmonologist and intensivist at Charleston Area Medical Center in West Virginia. Continuing education for this episode CME credit provided courtesy of Academic CME. can be elevated by diuresis* Serum albumin/pleural > 1.2* Pleural LDH/serum LDH > 0.6* glucose <40 (or 60?) glucose <40 (or 60?),
All of the secondary outcomes (mortality at 90 days, misdiagnoses, hospital length of stay, ICU admission rate, ICU length of stay, and quality of life) also did not show a statistical difference between the intervention group and the control group (SGEM#207). It needs to change physician practice for the better.
We discuss the field of rehabilitation psychology, and how it can help patients with persistent critical illness, with Dr. Megan Hosey (@DrMeganHoseyPhD), clinical psychologist and assistant professor at Johns Hopkins School of Medicine, where she practices in the medical ICU. Delirium often dominates the patient experience of the ICU.
Date: April 25, 2024 Guest Skeptic: Missy Carter is a PA working in an ICU in the Tacoma area and an adjunct faculty member with the Tacoma Community College paramedic program. Reference: Tanner et al, A retrospective comparison of upper and lower extremity intraosseous access during out-of-hospital cardiac arrest resuscitation.
He is also director of their Outcomes After Critical Illness … Continue reading "Episode 26: ICU sedation, mobility, and delirium with Dale Needham" How to manage the intubated critically ill patient while keeping them awake, non-delirious, and mobile, with Dr. Dale Needham, FCPA, MD, PhD. More fentanyl is often needed early on.
Mechanical ventilation has a lot of nuance associated with it, but a lot of reference guides focus on care in the ICU. With both ER and ICU experience, this post acts as a quick […] The post Mechanical Ventilation Basics appeared first on EMOttawa Blog.
The biggest change has been the gradual replacement of diacetylmorphine (heroin) by fentanyl and other synthetic opioids. Along the same time, a veterinary sedative, xylazine , became popular in Puerto Rico in individuals who used injection drugs [3]. We treat with wound care and reserve surgical management only for limbs that are no longer viable.
Several studies have indicated that dosing with phenobarbital (PO or IV) is safe and effective at decreasing the need for escalating doses of benzodiazepines for EtOH withdrawal [1-6]. Because patients with hepatic encephalopathy experience excess GABA stimulation, they are very sensitive to GABAergic medications (e.g., 2017;35(7):1005-1011.
Polypharmacy is technically defined as taking five or more medications on a daily basis. Polypharmacy is increasingly becoming the norm among adults, due to several factors (an aging population, increasing numbers of medical problems, and increasingly complex regimens available to treat chronic disorders such as heart failure).
An overview of the role and contributions of a clinical pharmacist in the ICU, with Laura Means Ebbitt of the University of Kentucky, a clinical pharmacist specializing in colorectal/ENT surgery and critical care. Takeaway lessons A clinical pharmacist is a “knowledge pharmacist,” dispensing advice rather than medications.
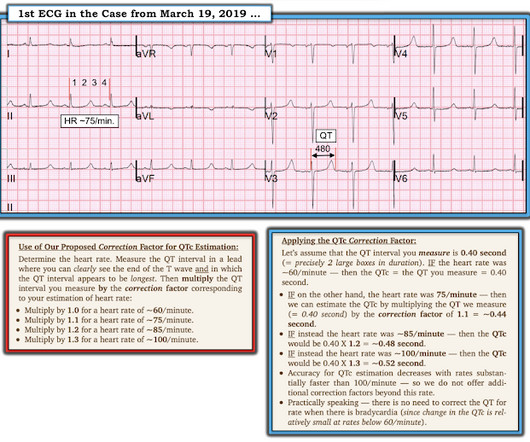
CASE CONTINUED She was admitted to the ICU. T-waves are quite tall and possibly peaked (HyperK?), but potassium returned normal. I do not see OMI here and all trops were only minimally elevated, consistent with either chronic injury from cardiomyopathy or with acute injury from sepsis. What is the QT interval? Bogossian et al. (1)
The use of direct oral challenges has been tried in the intensive care unit (ICU) setting to de-label patients. Koo et al showed that offering amoxicillin oral challenges to ICU patients with low-risk penicillin allergies. A pivotal study by Raja et al.
Her research interests include improving the diagnosis of urinary tract infections in children. Case: A 4-year-old girl comes to the emergency department complaining of pain with urination. She has not had any fevers or flank pain. You obtain a urinalysis that demonstrates 43 white blood cells, positive leukocyte esterase, and positive nitrites.
95% CI (1.46, 2.84)) and the need for an emergent intervention (aOR 1.38, 95% CI (1.15, 1.66)). 95% CI (1.46, 2.84)) and the need for an emergent intervention (aOR 1.38, 95% CI (1.15, 1.66)).
The idea behind abx is to prevent things like AOM and TSS but neither should be much of an issue with short term placement ICU Admission? Traditional teaching is that these patients are at risk for life-threatening bradydysrhythmias and should go to the ICU Literature here is non-existent.
For example a pt in the ED with sepsis, and a collapsible IVC, dry lungs and no peripheral edema is more likely to benefit from fluid than be harmed Take that same pt, with the same US and physical exam findings and make it 72-hrs later in the ICU after 6-10 L. There is no one dichotomous test that will tell you whether to give fluid or not.
The other common ICU indication is a free flap, a portion of tissue (potentially including skin, subcutaneous tissue, muscle, even bone) removed from a remote site and transplanted into the head and neck area, with vessels anastomosed. . * Takeaway lessons * Robotics has enabled much less invasive approaches to many head and neck procedures.
A temporary pacemaker was implanted, and she was admitted to the ICU with cardiogenic shock. She was worked as a full code, and ROSC was achieved. She was taken to the cath lab, where she was found to have 100% in-stent restenosis of the proximal LAD. Later the next day, she went into cardiac arrest again. She could not be resuscitated.
Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Sodium bicarbonate use during pediatric cardiopulmonary resuscitation: a secondary analysis of the icu-resuscitation project trial. Reference: Cashen K, Reeder RW, Ahmed T, et al. Pediatric Crit Care Med.
In our emergency department, the RTs do not spend a lot of time going around measuring cuff pressures and usually save that until the patient reaches the ICU. Another minor difference is that the gastric balloon in the Minnesota tube holds 450-500 ccs of air, while the SB gastric balloon holds 250 ccs of air [2].
PMID: 37611862 Clinical Question: In patients treated in the ICU, can a protocol of peripheral IV catheter vasopressors safely reduce the number of days of CVC use and frequency of placement? of patients not requiring CVC insertion. REBEL EM: Peripheral Vasopressors – Safe or Dangerous?
Brandon walks Bryan through a case of new, unexplained hypotension in the ICU, with a focus on approaching shock, the use of POCUS, and risk stratifying unexplained problems. from sepsis), while among the most common causes of hypotension in the ICU, is a diagnosis of exclusion.* Distributive shock (e.g.
Mild to moderate DKA represents a subgroup of patients that often require admission to the ICU due to hospital policies not allowing insulin infusions outside of this clinical setting. to 19.3hrs); Reduction by 3.6hrs ED LOS was shorter for the SQuID cohort ICU Admissions: SQuID & Traditional (Post Intervention): 42.9%
Are antipsychotic (neuroleptic) agents a good treatment for ICU delirium? Are antipsychotic (neuroleptic) agents a good treatment for ICU delirium?* Bryan’s off this week, so Brandon flies solo to explain five wrong-headed notions that many people believe without thinking about them.
PMID: 38215002 Clinical Question: In critically ill adults in the ICU is noninvasive blood pressure (NIBP) monitoring similar (≤10% difference) to invasive arterial blood pressure (IABP) monitoring? which was not statistically significant [2]. The biggest issue with this trial is there was only one blood pressure done per patient.
So, from the ultra broad topic of AKI in the last podcast to the super specific question of when we should pursue an open lung biopsy in an ICU patient. So, from the ultra broad topic of AKI in the last podcast to the super specific question of when we should pursue an open lung biopsy in an ICU patient.
Looking at the workflow of a fresh post-op open heart surgery patient, as well as what to do when it devolves into cardiac tamponade, with (returning) guest Brendan Riordan, cardiothoracic ICU PA (@concernecus) at the University of Washington, and his NP colleague Kris Ramilo (@krsrml0). Audio quality was a bit dodgy in this one; sorry all!–eds.]
1: Macrolides and Long-Term Survival in ICU Patients with Community-Acquired Pneumonia Spoon Feed Empiric macrolide therapy was associated with improved six and twelve-month survival among ICU patients with community-acquired pneumonia (CAP). Originally published at JournalFeed , a site that provides daily or weekly literature updates.
Welcome to the first episode of the Broomedocs podcast for 2025. Justin and I are back for more nerdy goodness to make you smarter in the Resus room, or at a pub trivia night more likley… wether it is about salt correction, dissection or infection we can help you out! Listen in and learn! Dimer is useful in the low risk group. Emerg Med J.
A look at rehabilitation and mobility in the critically ill, from the perspective of our skilled therapists—with Heidi Engel, PT, DPT of UC San Francisco, long-term provider of acute care therapy, researcher in ICU rehabilitation, and founding member of the SCCM’s ICU Liberation program. Natural, indirect light is better.*
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
We look at the rib fracture patient requiring ICU admission, including a discussion of surgical repair, with Dr. Ron Barbosa (@rbarbosa91), Portland trauma surgeon and SICU director at Legacy Emmanual Medical Center. ICU admission in rib fracture patients is still most often a matter of clinician judgment and bed availability.*
Spoon Feed Advanced statistics emulating clinical trial protocols from an ICU database did not identify consistent differences in 30-day mortality when ICU patients were intubated early (within 8 hours of admission) or late (after 48 hours). Originally published at JournalFeed , a site that provides daily or weekly literature updates.
Signs of baseline and/or new RV strain, such as reduced TAPSE, septal bowing, etc, as well as pericardial effusion, suggest a poor reserve for the stresses of their new ICU course. Click here to claim your CME credit! Find us on Patreon here! Avoid intubation if at all possible, as this can easily provoke cardiovascular collapse. .
With Kali Dayton, ACNP-BC ( @HomeIcu ), critical care nurse practitioner and host of the Walking Home from the ICU podcast, where she looks closely at these issues, including interviews with survivors describing their ICU experiences. Limited activity is better than none. Ventilator settings are rarely a contraindication to mobility.
How to take the well-resuscitated critically ill patient, get fluid out of them, deescalate their antibiotics, wean their sedation, reduce vent support, extubate, and get them out of the ICU—with Dr. Matt Siuba (Twitter: @msiuba), an intensivist at the Cleveland Clinic with an abiding interest in “zentensivism,” the art of doing less.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content