This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
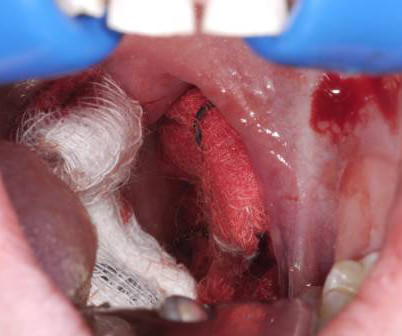
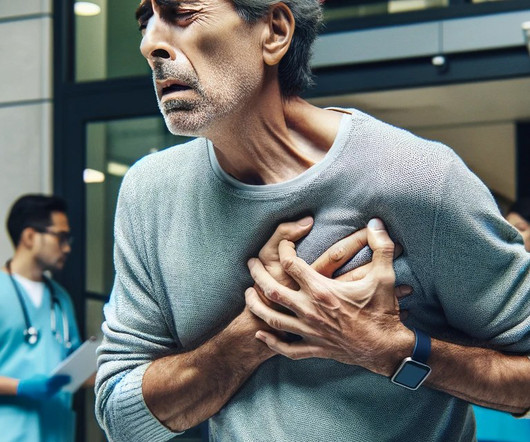
The literature suggests that approximately 85 percent of these cases require procedural source control in the operatingroom, highlighting the importance of expediting transport arrangements. Her vital signs are normal, except for a heart rate of 115 bpm. Its going to take time to get her to a tertiary center. CREDIT: Dr. P.
95% CI (1.46, 2.84)) and the need for an emergent intervention (aOR 1.38, 95% CI (1.15, 1.66)). 95% CI (1.46, 2.84)) and the need for an emergent intervention (aOR 1.38, 95% CI (1.15, 1.66)).
What are the best strategies to efficiently get the patient in cardiogenic shock to definitive care, whether that be the cath lab or the operatingroom? How can we best pick up occult cardiogenic shock before it floured shock kicks in? Which patients with acute heart are safe to send home in general?
On this 10 year anniversary, we chose to throw this one back in the oven to include some even more delicious data on cuffed endotracheal tube (ETT) use. Cuffed Endotracheal Tubes: Evolution of Thought and Technology Why did we historically use uncuffed endotracheal tubes in kids younger than 8? 0.41), p < 0.001. 1.70) and 0.78 (0.46–1.35),
Greg Mielke, Preceptis Medical: Today, approximately one million children undergo ear tube procedures annually in an operatingroom in the United States. However, ear tube procedures conducted in an operatingroom under general anesthesia can be traumatic for both children and parents well before the procedure begins and after it ends.
Children in the validation cohort were admitted to the intensive care unit or operatingroom less frequently than those in the derivation cohort. Cervical spine injuries are a rare but serious finding following blunt trauma, affecting around 1-2% of presentations. What is the problem? What did previous studies show?
Might his examination be enough to convince the urologists to take him straight to the operatingroom without a preceding diagnostic ultrasound? Melissa is passionate about clinical and translational research and focuses most of her work on the use of capnography or end-tidal carbon dioxide monitoring.
Patients may arrive with other concomitant injuries such as head or spine injuries and may be critically ill. Imaging CT scan of the abdomen and pelvis with IV contrast or CT angiogram of the abdomen is the imaging modality of choice. Majority of RPH will stabilize on their own and not require intervention. Mortality can varies between 5-20%.
Takeaway lessons * Trauma patients who are hypotensive or otherwise unstable should be assumed to be bleeding, bleeding, bleeding until proven otherwise, and should have a very low threshold to proceed directly to the operatingroom for exploration.* Operative prep for exploratory laparotomy is usually from the chin to the knees.
Surgical Repair of Hip Fractures: Demonstrating effective care prioritization, 94% of older adults with hip fractures were moved to the operatingroom within 24 hours. This rapid intervention reduced complications and highlights the need for maintaining and improving such protocols.
They concluded that propofol is safe, particularly in short-term sedation, but should be used with caution outside of the operatingroom, given some of the potentially severe adverse events (including PRIS) seen. Mortality associated with PRIS has been estimated to be around 33% and becomes even higher if the diagnosis is delayed.
Epinephrine – 10ug/mL, 10mL syringe Phenylephrine – 100ug/mL, 10mL syringe Phenylephrine bolus doses from 100-200ug and epinephrine 10-20ug administered every 2-5 minutes pursuant to provider order Inclusion Criteria: Adults age >18 years old Received at least one bolus dose of phenylephrine or epinephrine pre-filled syringes Exclusion (..)
IPPS Proposed Rule by the Centers for Medicare & Medicaid Services The Age-Friendly Hospital measure assesses hospital commitment to improving care for patients 65 years or older receiving services in the hospital, operatingroom, or emergency department (pg.
The standard care in North America for post-traumatic EDH involves decompressive craniotomy or trepanation via a burr hole, typically performed in an operatingroom by neurosurgery teams. EDH accompanies up to 4% of adult head injuries, leading to 10% mortality in adults and 5% mortality in children. What are the key takeaways? (1)
His vital signs were within normal limits except for a respiratory rate of 23 with a room air pulse oxygen in the upper 90s. On hospital day 2, he was taken to the operatingroom for surgical rib fixation. The splint consisted of a folded blanket placed over the mobile segment and held in place with tape.
During Orientations, new crew members must do a minimum of 10 live intubations in the operatingroom before being cleared to intubate in the field. Let’s start with what this study is This study is of a single service with three (3) bases in southeastern Wisconsin and northern Illinois. Data was pulled from June 2013 to June 2018.
In 1901, UVA opened its first hospital with 25 beds and three operatingrooms. The University of Virginia (UVA) School of Medicine was founded in 1819 by Thomas Jefferson and is one of the oldest medical schools in the United States. This volume and variation presented challenges when attempting to staff the ED appropriately.
First ED-based study to evaluate how operational effects such as crowding can affect patient care in the form of LPV Included ARDS criteria relating to the usage of LPV in the ED allowing evaluation as to whether patients with ARDS were more likely to receive LPV settings. of patients left the ED on TV settings of 450 mL and 36.1%
18 The finger is inserted through the stoma alongside the endotracheal tube and, while 90 percent success rate has been reported with this method in controlling bleeding, the pressure must be maintained until the patient is transferred to the operatingroom. In one case series of seven patients, the average patient age was 15.7
Type A AoDs generally require an emergent trip to the operatingroom as soon as they are identified to reduce the likelihood of a terrible outcome. Symptoms may include more severe chest pain radiating to the back, loss of consciousness, or symptoms of stroke if the blood supply to the brain is affected.
4 Pain is the most common reason for presentation in the early post operative period. 5 Highest risk of dislocation early in the post operative course due to laxity of the soft tissue after surgery. 6 Hip flexion or adduction in the early post-operative period can cause atraumatic dislocations (typically avoided for 6 weeks post-op).
There have been some studies in various clinical settings (operatingroom, critical care and pre-hospital) that have demonstration benefit of apneic oxygenation. As such it has enjoyed widespread adoption throughout the Emergency Medicine and Critical Care world.
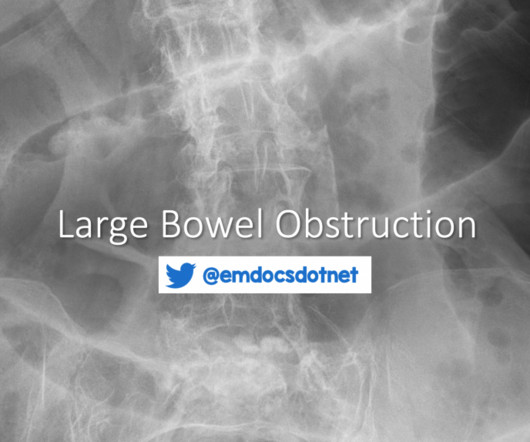
7 While post-operative adhesive disease is also a risk factor, it is far less commonly implicated in LBO compared to SBO. 7 While post-operative adhesive disease is also a risk factor, it is far less commonly implicated in LBO compared to SBO. 2-3 Risk Factors CRC is the most common underlying etiology of LBO.
Thick, dry, and calloused skin of a construction worker can have as much as 100 times more resistance than the previous example. 4 This may lead to more heat dissipated at the skin with impressive burns to skin, but less transmission of electricity to deeper tissues. High voltage” is defined by texts as 600 V and 1,000 V. Click to enlarge.)
What They Did: Double-blind, randomized, placebo controlled trial that ran from October 2019 through January 2024 Multinational study conducted at 22 centers in three European countries 3512 patients were enrolled and before surgery eligible patients were randomly assigned to one of the following two groups Amino Acid Group: 10% Isopuramin at a dose (..)
Some states and programs also require EMT students to complete 24 to 48 hours of clinical time working in an emergency room and/or ambulance under the supervision of a certified EMT, paramedic, or registered nurse. The CPR course typically takes 4 to 8 hours to complete.
The patient was admitted to the obstetrics service and underwent spinal anesthesia in the operatingroom to manually reduce the uterus. She had urinary dribbling when standing and leaning forward. She denied fevers, back pain, saddle anesthesia, numbness, or weakness in the extremities. A pessary was inserted during that procedure.
This is certainly outside the realm of intensive care but remains a somewhat magical act that my surgical and anaesthetistic colleagues perform in the operatingroom. These are now recently developed for the lungs which allows donor lungs to be perfused and even optimised prior to implantation.
Diagnosis is clinical and challenged by overlap with more superficial skin infections (i.e. cellulitis) and the need for thorough examination of the genital region. 1 His description of cases of life-threatening infections in the perineal, genital or perianal regions were thought to be idiopathic in previously healthy men.
A search for Brazilian Butt Lift (BBL) on any social media platform will yield thousands of before-and-after images, faja sales, operatingroom videos, recovery tips, and patients praising their plastic surgeon. Or Helly Larson describing the first week after her Miami BBL as “absolute hell” to a Vox reporter.
4 This is the framework the ED resuscitationist should be operating under, as hemodynamically unstable pelvic trauma patients require a different approach compared to stable patients who will undergo CT, routine pelvic fixation, and definitive surgical repair. Conceptually, pelvic ring fractures are similar to breaking a hard pretzel.
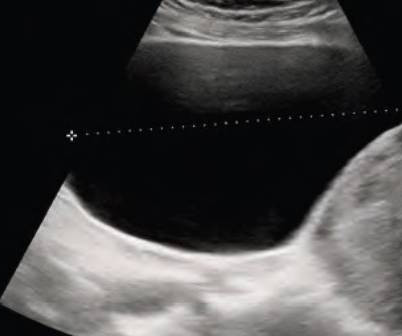
One systematic review of 1283 patients showed that if you got to the operatingroom within 6 hours, you had a 97% chance of saving the testicle. The gold standard – the only way you will really know if there is a torsion or not – is to take a look in the operating theatre. How do you diagnose torsion?
The patient was taken to the operatingroom for dilation and curettage and was discharged the following day. She endorsed worsening nausea and vomiting over the past two weeks. She has been sexually active since her last encounter. She denied abdominal pain, pelvic pain, cramping, dizziness, shortness of breath, or fevers.
However, we may need to temporize the patient before they can get to an operatingroom. The placenta wants to connect to the uterine wall at a location that allows good communication between the two. This causes the placenta to look elsewhere for an attachment site with better circulation. volume resuscitation is necessary.
Other exceptions are patient refusal, patient death or immediate transfer to the operatingroom. The classic triad of abdominal pain, hypotension and pulsatile abdominal mass is present in less than 25 percent of patients. 2 Patients can present with back pain, or with focal neurologic signs such as numbness of the lower extremity.
Included patients from out-of-hospital, emergency department, intensive care unit, and operating-room intubations. Intubation performed in all settings (out-of-hospital, emergency department, ICU, and operatingroom). Randomized controlled trials or comparative non-randomized observational studies. airway scope).
Diagnosis: Diagnosis can be made based on clinical exam alone Physical exam Inability to close the mouth Garbled speech Drooling. Anterior dislocations: palpation of the TMJ can reveal one or both of the condyles to be anteriorly displaced in front of the articular eminence.
Video Laryngoscopy vs Direct Laryngoscopy for Endotracheal Intubation in the OperatingRoom: A Cluster Randomized Clinical Trial. PMID: 36895888 Yeah, we get it, video is better Ruetzler K, Bustamante S, Schmidt MT, Almonacid-Cardenas F, Duncan A, Bauer A, Turan A, Skubas NJ, Sessler DI; Collaborative VLS Trial Group. N Engl J Med.
Epidemiology Amniotic fluid embolism (AFE) is an incredibly rare yet catastrophic pathology during which fetal debris and/or amniotic fluid enters the maternal central circulation in the third trimester of pregnancy or, most commonly, during the labor process. Regardless, she complains of sudden and severe shortness of breath.
Success at intubation likely takes more time and practice than other procedures, as shown in recent research on ED residents and their success rate at intubating, measured as a function of their total number of intubations (See Figure 1). Practice may not achieve perfection, but it will make you better. fiber optic through the nose).
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



































Let's personalize your content