This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Questions: What are the symptoms of second-generation antipsychotic overdose? How is second-generation antipsychotic overdose diagnosed? What is the treatment for patients who have overdosed on second-generation antipsychotics? 4 The specific incidence of second-generation antipsychotic drug overdose is unknown, however, 4.7%
Background: An update to our 2015 post on HIET for beta-adrenergic receptor and calcium channel antagonists overdose. Beta-adrenergic receptor antagonists (Beta blockers, BB) and calcium channel antagonists (calcium channel blockers) are common drugs that can produce profound cardiac depression and shock when taken in overdose.
Naloxone is a well-established medication used primarily for reversing opioid overdoses. Traditionally, naloxone has been used in cases of suspected opioid overdose where patients exhibit signs of severe respiratory depression or loss of consciousness (LOC). Today’s study looks at the role of naloxone in OHCA.
A 20-something presented after a huge verapamil overdose in cardiogenic shock. And she does not know that this is an overdose; she thinks it is a patient with chest pain!! Comment on High Dose Insulin and Calcium Channel Blocker Overdose I do not have any explanation for the ST-T abnormalities here. The initial K was 3.0
EDs are an important touch point for individuals with opioid use disorder (OUD), given the number of encounters for overdose and complications associated with drug use. Fentanyl test strips (FTS) have been suggested as one harm reduction strategy to reduce opioid overdose deaths. cm left forearm abscess.
Opioid overdose remains the leading cause of cardiac arrest due to poisoning in North America. Author: Brit Long, MD (@long_brit) // Reviewed by Alex Koyfman, MD (@EMHighAK) The American Heart Association 2023 Guideline for managing cardiac arrest or life-threatening toxicity due to poisoning was recently released. Top 10 Take Home Pearls 1.
Recently, xylazine has gained attention in the media with increasing reports of xylazine-related overdose deaths in patients. When combined with illicit opioids such as heroin and fentanyl, xylazine may increase the risk of fatal overdose given the augmented sedation and respiratory depression effects [2]. Published May 2023.
Do heroin overdose patients require observation after receiving naloxone? Do heroin overdose patients require observation after receiving naloxone? Opioids depress the heart rate and breathing and overdoses can result in death. The second new recommendation was about opioid overdose treatment. Clinical Toxicology 2017.
The EMS crew observes drug paraphernalia and suspect an intravenous (IV) opioid overdose. Background: There have been close to 400,000 deaths from an overdose involving any opioid (prescription and illicit opioids) between 1999 and 2017. [1] Wave 2: Rapid increase in overdose deaths involving heroin starting in 2010.
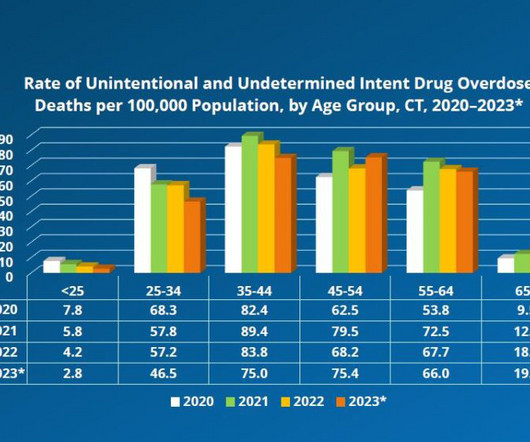
I have called the time on a number of her neighbors in this building, some of them victims of overdose. While the news often focuses on the dangers of fentanyl to youth, what I see on the street and what the data shows is that the group that is seeing the biggest increase in overdoses is the elderly. of all overdoses to 11.1%.
These posts have been flagged by and agreed upon by AIR Board members as worthwhile, accurate, unbiased, and appropriately referenced despite an average score. Take the AIR Toxicology Module at ALiEMU Interested in taking the AIR quiz for fun or asynchronous (Individualized Interactive Instruction) credit? Please go to the above link.
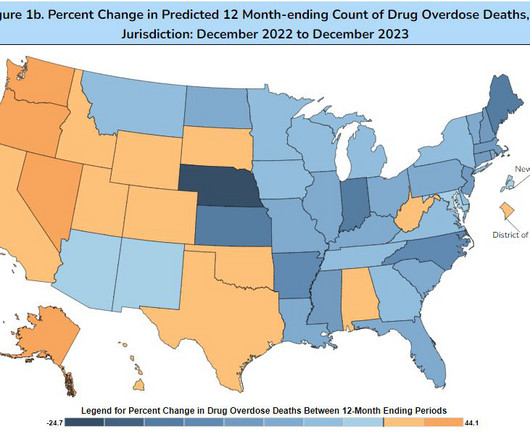
Is the decline in drug overdose deaths more related to the increased availability of naloxone, improved treatment for people who use drugs, or changes in the street drug supply, which while still quite toxic may be less so due to adulteration with other chemicals? A recent article in NPR, The pipeline of deadly fentanyl into the U.S.
Drug overdose deaths are down 3.1% 107,543 people died of drug overdoses in 2023 down from 111,029 in 2022. Here in Connecticut, drug overdose deaths have been decreasing for the last two years (down 14% in 2023 from the 2021 high). Ten years ago when I responded to an overdose, I was the only one carrying naloxone.
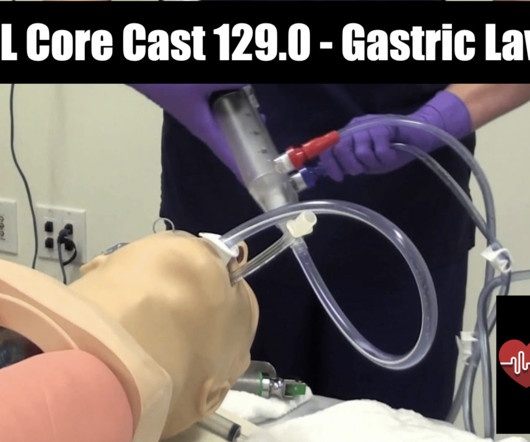
Take Home Points Orogastric lavage may still play an important role in treatment of the overdose patient. Strongly consider orogastric lavage in a patient who has taken an overdose of drugs that are particularly toxic, suspected extreme doses associated with high morbidity/mortality and do not have easily available and effective antidotes.
In 2023, EMS clinicians responded to 236,000 calls for suspected opioid overdoses, representing nearly 2% of all EMS calls nationwide. The 2024 ESO EMS Index reveals that 82% of patients with suspected opioid overdoses received naloxone, a medication that can reverse opioid effects. Gender disparities were also found.
Unlike other methods, such as firearms, hangings, intentional overdoses, and cutting, chemical suicides tend to linger in the area where the act was committed. TRIGGER WARNING: TOPICS OF SUICIDE MAY BE HARD FOR SOME PEOPLE TO READ ABOUT. THIS ARTICLE IS COVERING THE MEDICAL ASPECTS OF CHEMICAL SUICIDES.
A meaningful portion of patients used opioids for pain management, with a subset identified at high risk for opioid misuse or overdose. Results: Analysis of 435 patient screenings revealed notable findings. While most patients stored medications safely, disposal practices varied, highlighting a need for education and intervention.
With the 2014 CDC declaration that prescription drug overdose is one of the five top health threats, there has been a movement away from opioids as the mainstay of pain management for rib fractures [6].
Questions: What are the clinical manifestations of bupropion overdose? How is bupropion overdose treated? How long should a patient be observed after a bupropion overdose? 1 In addition to intentional overdoses, there are multiple case studies of abuse (ingestion, insufflation, injection). hours, SR 3 hours, XL 5 hours.
Connecticut opioid-related deaths declined for the second year in a row, down 14% from their 2021 high of 1431 opioid deaths, according to the latest statistics from the Connecticut Office of the Medical Examiner (OCME). Opioid deaths represented 92% of all overdose deaths in Connecticut.
Xylazine is a veterinary sedative that has been increasingly implicated in overdose deaths throughout the United States. percent of all overdose deaths in 2020. 1 Known by street names such as “tranq,” “tranq-dope,” or “zombie drug,” xylazine is increasingly found in patients with opioid overdose. Drug and Alcohol Dependence.
IV is usually recommended due to faster onset, ease of administration, and shorter protocol duration. These local protocols vary from the labeled dosing; contacting and using your local poison center’s protocol is recommended. These local protocols vary from the labeled dosing; contacting and using your local poison center’s protocol is recommended.
What are the treatment options for a benzonatate overdose? 7) Overdose literature review timeline: In 1986, the first two benzonatate fatalities were reported in the literature: a choking infant and an intentional overdose in a teenager. (8) Questions: What is benzonatate’s mechanism of action?
Broselow-Luten System: Supportive Data Physician estimates of weight can underdose children by 49% or overdose by up to 116%. Reduces dosing errors during resus, up to 33.88%. Recommended by ATLS and PALS. Krug 2007] What If the Child is Obese or Emaciated? of children; PAWPER predicted within 10% for 89.2% Validation study done in Italy.
Case: A 24-year-old male presents to the emergency department (ED) after a fentanyl overdose. You are interested in seizing this opportunity to offer some type of help to this patient to prevent another opioid overdose in his future. He is successfully resuscitated using naloxone and is stable after an observation period.
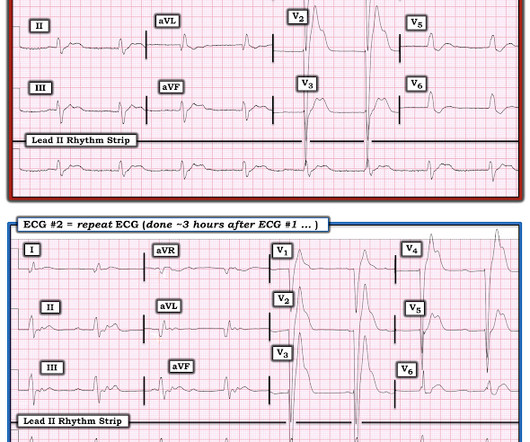
He had been smoking an opiate and suddenly collapsed. He was ventilated with BVM on arrival. He awoke with naloxone. This EKG was recorded as part of a standing order for critical care. He denied any CP or SOB. An EKG was repeated at 5 minutes The T-wave is less hyperacute. Maybe there is some spontaneous reperfusion? It does not radiate.
Background Information: Opioid overdose deaths have been increasing in the past twenty years. The national number of overdose deaths from any opioid has increased 62.5% In addition, buprenorphine has a lower risk of death from overdose when compared to methadone (2). mg tablet) 1 Buprenorphine 0.5
While it is generally safely used, overdose can result in the development of liver failure due to APAP’s hepatotoxic metabolites. Hepatic necrosis is preventable in overdose with timely administration of N-acetyl-cysteine (NAC) which restores glutathione reserves, allowing for safe excretion of these hepatotoxic metabolites.
Exclusions: Non-English speaking and no translator with patient, violent behavior, intentional overdose, needlestick injury or sexual assault, previously enrolled, presented for a scheduled revisit, direct transfer to an admitting service, fast track patient, left against medical advice prior to seeing physician and pharmacist.
University of Maryland Department of Emergency Med
APRIL 10, 2023
Glucagon therapy in beta blocker and calcium channel blocker overdose is controversial and no high level evidence is available to support or. Click to view the rest
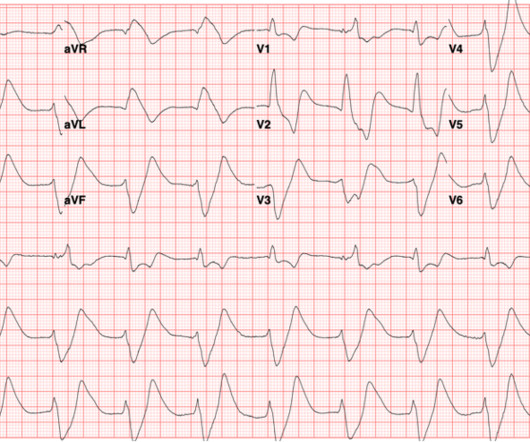
As demonstrated by Dr. Smith in his above discussion — Application of the ECG findings in Figure-1 to today's clinical scenario ( ie, marked sinus tachycardia in this younger adult with drug overdose and respiratory arrest ) — provides an immediate and much more likely explanation for DSI than trying to postulate ACS.
Sometimes this can be used to our advantage, like when we need to give subcutaneous fluids to a dehydrated patient without an IV, or when we need to give SQ medications for things like Sulfonylurea overdose , Hereditary Angioedema , or DVTs. Shen 2013, Nickerson 2014, Scolaro 2016 ] Singh et al proposed an algorithm to guide treatment.
Hyperkalemia, Sodium-channel blockade (ex: tricyclic acid overdose), Pre-excitation syndromes (ex: Wolff-- Parkinson-White syndrome), Aberrant conduction (ex: bundle branch blocks), Ventricular-Paced beats, Hypothermia, Ventricular ectopy What immediate interventions should be considered based off of this initial ECG?
Right as you’re making your bunk you get dispatched for a reported overdose with police enroute, no further information. We go into it with preconceptions of what to expect: “It’s a simple heroin overdose, we’ll wake them up and they’ll refuse, then we’ll go back to bed”. We’ve all had this call before, right? You can bet that I was!
7,10 Contraindications include asthma, chronic obstructive pulmonary disease (COPD), genitourinary or gastrointestinal obstruction, or if there is suspected or confirmed tricyclic antidepressant (TCA) overdose. No specific laboratory finding confirms if a patient has ingested a plant. Physostigmine does not reverse seizures or dysrhythmias.
An inciting event will typically push them over the edge into BRASH syndrome: Dehydration Hypotension from sepsis or another condition GI illness Dosage increase of a chronic medication (e.g., beta blocker) New medication (e.g., NSAID or potassium sparing diuretic) Ask the following: Is there mild hyperkalemia? Is there some renal injury?
Hyperkalemia, Sodium-channel blockade (ex: tricyclic acid overdose), Pre-excitation syndromes (ex: Wolff-- Parkinson-White syndrome), Aberrant conduction (ex: bundle branch blocks), Ventricular-Paced beats, Hypothermia, Ventricular ectopy What immediate interventions should be considered based off of this initial ECG?
For instance, they investigated it in the context of acetaminophen overdose in mice, which results in liver damage. However, delivering it to the gastrointestinal tract to treat inflammatory diseases, such as colitis, is a challenge. Carbon monoxide is typically considered a hazardous gas. .
Simple intoxications like baclofen overdose can cause incredibly dense coma. . * Give thiamine indiscriminately and widely to patients with altered mental status; it is harmless and Wernicke-Korsakoff may fool you. Start with the history and meds. Inquire as to recent history of behavioral changes, neurologic phenomena, illness, etc.
Heart rate/rhythm: consider antidotes for brady/tachy-arrhythmias, and for sinus tachycardia consider fluids for vasodilation and benzodiazepines for agitation. Electrical conduction and axis: consider sodium bicarb for QRS > 100 especially if RBBB or terminal rightward shift, and magnesium for QTc> 500.
Severe acute traumatic coagulopathy = PT >1.5 to 3.33; P = 0.72 NOT STATISTICALLY SIGNIFICANT Also no difference in individual components given Thromboembolic Events: 4F-PCC: 35% Placebo: 24% Absolute Diff: 11%; 95% CI 1 to 21% Relative Risk 1.48; 95% CI 1.04 to 2.10; P = 0.03 Severe acute traumatic coagulopathy = PT >1.5 to 3.33; P = 0.72
Acute iron overdose can cause anion gap acidosis, GI symptoms including bleeding, and shock and an overal critically ill presentation. Acute iron overdose can cause anion gap acidosis, GI symptoms including bleeding, and shock and an overal critically ill presentation. Buy your merch here! Click here to claim your free CME credit!
Unfortunately, most cases are not so simple, with half of them being unintentional overdoses, many with a delayed presentation; some with delayed-release formulations, combined formulations, or co-ingestions, and some in patients with co-morbidities—all factors that make recognition and management more challenging.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content