This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
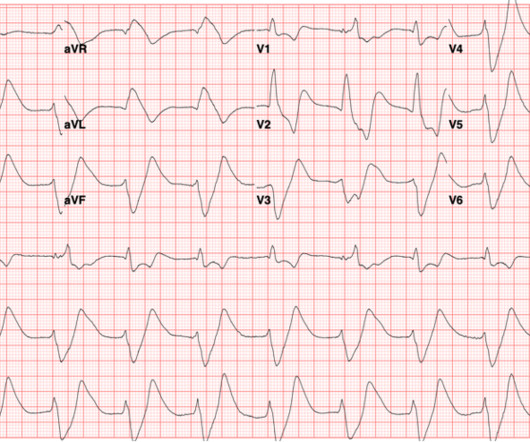
Hyperkalemia, Sodium-channel blockade (ex: tricyclic acid overdose), Pre-excitation syndromes (ex: Wolff-- Parkinson-White syndrome), Aberrant conduction (ex: bundle branch blocks), Ventricular-Paced beats, Hypothermia, Ventricular ectopy What immediate interventions should be considered based off of this initial ECG?
Hyperkalemia, Sodium-channel blockade (ex: tricyclic acid overdose), Pre-excitation syndromes (ex: Wolff-- Parkinson-White syndrome), Aberrant conduction (ex: bundle branch blocks), Ventricular-Paced beats, Hypothermia, Ventricular ectopy What immediate interventions should be considered based off of this initial ECG?
Metabolism of ester anesthetics is by plasma cholinesterase, whereas amides are metabolized by the cytochrome P450 system in the liver. [6] 6] Action of local anesthetics is dependent upon the molecule crossing the plasma membrane in a unionized form. [2] 2] This linking group can be either an amide (e.g., lidocaine) or an ester (e.g.,
Severe acute traumatic coagulopathy = PT >1.5 to 3.33; P = 0.72 NOT STATISTICALLY SIGNIFICANT Also no difference in individual components given Thromboembolic Events: 4F-PCC: 35% Placebo: 24% Absolute Diff: 11%; 95% CI 1 to 21% Relative Risk 1.48; 95% CI 1.04 to 2.10; P = 0.03 Severe acute traumatic coagulopathy = PT >1.5 to 3.33; P = 0.72
DEG is rapidly absorbed when ingested and can reach peak plasma and brain tissue concentrations within four hours of ingestion. Elimination half-life data is not well established but increases in larger overdoses and as renal injury begins to occur. 1 Clinical Questions: When should a clinician suspect diethylene glycol (DEG) toxicity?
There have been documented cases of overdose, and of note, there is no known antidote. Given the fact that he has not had these headaches before and has diffuse symptoms including weakness, lab work and head imaging are obtained. There were no acute findings on head CT.
This is pathognomonic of hyperkalemia (I suppose it could be due to a massive overdose of a sodium channel blocking drug, maybe). Internal potassium balance and the control of the plasma potassium concentration. A prehospital ECG was recorded: Limb leads: Precordial Leads What is the therapy? Medicine (Baltimore) 1981;60:339-54].
Background: Fentanyl has contributed to a significant increase in drug overdose deaths in recent years. A prospective study of 453 patients who were admitted after receiving naloxone reported life-threatening complications in over 1% of heroin-overdosed patients. When should a naloxone infusion be considered? 2mg* 2 5 0.5-1.5
He was admitted for a suspected kratom overdose and acute kratom withdrawal. 7 Most of the difficulty in identifying patients who have overdosed or are in acute withdrawal from kratom comes from the inability to test for it in commercial assays of blood or urine. A dexmedetomidine (Precedex) 400 mcg in 0.9 2022;23(1):4-9. J Med Chem.
Historically, iron toxicity and exposure affected children in unintentional overdose disproportionately. 1 The incidence of iron overdose and iron ingestion related deaths has significantly decreased over time, likely attributable to federal regulation. In severe toxicity, hematemesis, melena, or hematochezia may occur.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












Let's personalize your content