This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Let’s consider Inborn Errors of Metabolism Presenting in the ED : Inborn Errors of Metabolism: Basics Common Presentations, Uncommon Kiddos For the child with lethargy, vomiting, acidosis, hypoglycemia , organomegaly, or cardiopulmonary arrest remember to consider Inborn Errors of Metabolism (IEM) on your DDx. Kid with Known diagnosis?
First line therapies for anti-NMBDA receptor encephalitis consists of… High dose steroids , IVIG, and PLEX – Therapeutic plasma exchange Only 50% of patient’s respond, and will require second line therapies such as Rituximab. Make sure to consult your friendly neighborhood pediatric neurologist and/or rheumatologist!
sodium chloride), and balanced crystalloid solutions, meaning those with a chloride composition closer to plasma such as lactated ringer’s or Plasma Lyte 148. Then, the BaSICS trial (a multicentred RCT done in 75 Brazilian ICUs) came along and compared saline to Plasma-Lyte at what the authors deemed slow and fast infusion rates.
The paramedic asks you, “we have saline, and we also have red-cells and this fancy new lyophilised plasma. Should we give our shocked patient saline or plasma / red cells en route to the ED?” It was a pragmatic, randomised, single-centre trial done at the Denver looking at the use of plasma in the prehospital setting.
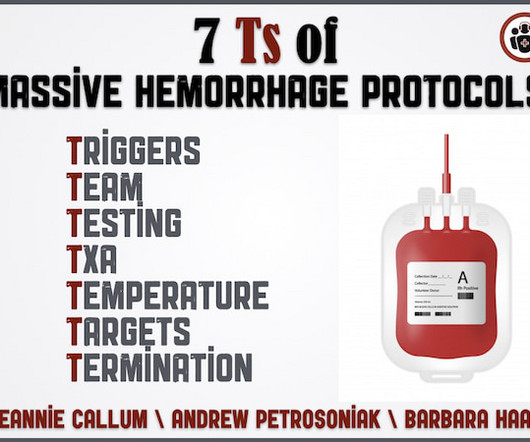
Until the results of lab testing come back and hemorrhage pace is slowed, what ratio of plasma to RBCs should we target? Once the dust settles, what do we need to tell the patient and/or their family about the consequences of being massively transfused? What should be the lab resuscitation targets? How do we mitigate the risk of hypothermia?
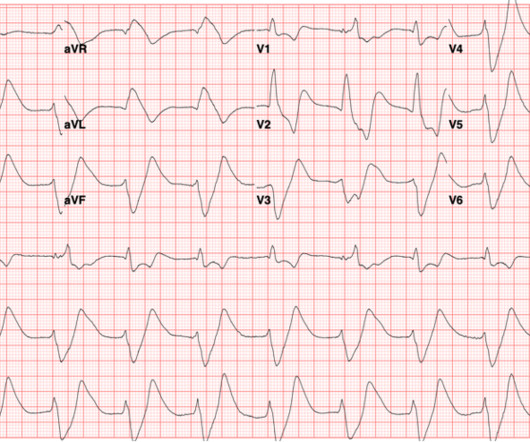
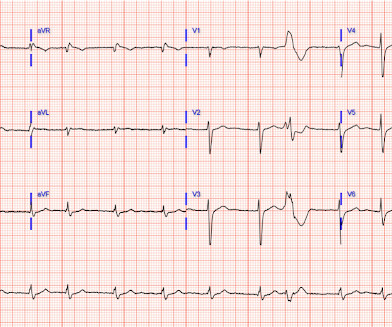
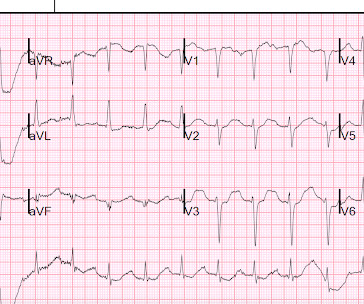
Hyperkalemia Cardiac conduction partially depends on a gradient of lower extracellular (plasma) potassium levels and higher intracellular potassium levels. The patient was admitted to the medical intensive care unit and emergent underwent dialysis. His EKG on discharge is shown below.
Bradykinin Mediated Plasma globulins called kininogens release bradykinin and cause vascular permeability. Image: ( Morgan 2010 ) Features Absence of urticaria and pruritus Insidious onset (24-36 hours) ACE Inhibitors Inhibition of ACE hinders the degradation of bradykinin and can lead to idiosyncratic angioedema.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
Hyperkalemia Cardiac conduction partially depends on a gradient of lower extracellular (plasma) potassium levels and higher intracellular potassium levels. The patient was admitted to the medical intensive care unit and emergent underwent dialysis. His EKG on discharge is shown below.
Necrobiosis Lipoidica – This patient had a previous skin biopsy with histopathologic changes demonstrating a granulomatous dermatitis involving the dermis and subcutaneous tissues with necrobiosis of collagen and inflammatory infiltrates of lymphocytes and plasma cells consistent with a diagnosis of necrobiosis lipoidica.
Various assistant/tech roles around the hospital/Plasma Donation Centers I personally became an Anesthesia Technician at Northwestern solely off of my experience as a paramedic and have been fortunate to bring on coworkers who were EMT students of ours. It opens many doors in various industries.
Background Around 6 million people in the U.S. 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. Background Around 6 million people in the U.S. Background Around 6 million people in the U.S.
(Tavasoli 2018, Wolf 2012) More common in adults; children comprise 20% of total cases (Pidcock 2007, Wang 2019) Bimodal age distribution (Absoud 2016) Children < 5 years Children > 10 years Symptoms evolve over 2-4 days and peak at 5-6 days (Absoud 2016) ATM may occur alone OR as part of another disorders (e.g.
Don't forget beta agonists in the treatment of hyperkalemia: Terbutaline and Albuterol for Lowering of Plasma Postassium (includes many abstracts) The below abstracts show that beta 2 adrenergic agonists are effective at treating hyperkalemia. Both together are VERY likely to be due to hyperkalemia. Is This a Simple Right Bundle Branch Block?
In contrast, protamine could be used for heparin and LMWH reversal and vitamin K, fresh frozen plasma and prothrombinase complex concentrate could be used to reverse coumadin ( Hunt and Levi BMJ 2018 ). Level A One of the concerns clinicians had with DOACs was there was no way to reverse these new anti-coagulants when they were introduced.
3 Measured in analytical testing : Laboratories measure plasma concentration using osmometers which measures values as a function of kilograms of solvent. Choice of the best equation for plasma osmolality calculation: Comparison of fourteen formulae. Validation of equations used to predict plasma osmolality in a healthy adult cohort.
Metabolism of ester anesthetics is by plasma cholinesterase, whereas amides are metabolized by the cytochrome P450 system in the liver. [6] 6] Action of local anesthetics is dependent upon the molecule crossing the plasma membrane in a unionized form. [2] 2] This linking group can be either an amide (e.g., lidocaine) or an ester (e.g.,
Plasma half-life of the F(ab’) 2 antivenom is significantly longer at 5.5 However, in 2015 crotalidae equine immune F(ab’) 2 (ANAVIP®) was approved by the FDA for rattlesnake envenomations, and distribution of this antivenom began in 2018. This size difference may lead to differences in the pharmacokinetic profiles of the two antibodies.
You may consider remdesevir or convalescent plasma at this point in the science, but don’t expect too much effect.* .* Worsening tachypnea, distress, and ventilatory (not hypoxic) failure are a marker to upgrade care and/or intubate a borderline COVID patient.* Prone early, when the lungs are still recruitable and salvageable. .*
Plasma free hemoglobin levels may be a useful marker that changing your oxygenator could improve gas exchange.* Cannulation can be done by whomever is skilled and trained, such as cardiac surgery, trauma surgery, trained intensivists, etc.* Anticoagulate most patients on VV ECMO with heparin to a PTT of 45-55.
This time the tonicity is high from something else such as high glucose or mannitol drawing water from cells into plasma. A normal sane and functioning kidney will try and lose water to conentrate the plasma in order to bring the sodium back up to normal, in other words the kidney should be producing a dilute urine with a low osm.
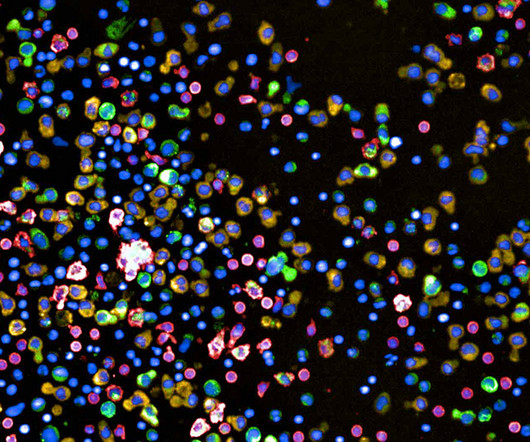
Red cells are healthy monocytes, green and yellow are plasma cells. In such cancers, finding the right drug or drug combination for a given patent is critical. The approach involves seeding the cancer cells into 384-well plates, and then placing different drugs or drug combinations into each well.
If it’s rising too quick it’s often because the patient is losing lots of water through the kidneys which concentrates the plasma raising the Na in the blood. But as we all know in critical care we often work with less than ideal information and have to begin treatment while the diagnostic process is ongoing.
On the other hand, lymphoid cells have a much smaller and narrower family tree differentiating into different types of lymphocytes and plasma cells. This is a cancer of plasma cells which are the grown up and left home versions of B lymphocytes. They are also distinct in histology and outcomes from the solid organ malignancies.
Author: Natalie Bertrand, MD Editor: Naillid Felipe, MD Background: Definition: adverse reaction to blood product administration Incidence: more common in children than adults, except for delayed hemolytic transfusion reactions Allergic (non-anaphylaxis) – Platelets 1-3%; RBCs 0.1-0.3% mg IF requiring IM Epi >3x, switch to IV Epi, 0.05-0.1
For patients on VKAs to prevent stroke in nonvalvular atrial fibrillation who require reversal, 4-factor prothrombin complex concentrate (PCC) is preferred to fresh frozen plasma (FFP) because of the rapidity of INR reduction (Conditional recommendation, very low-quality evidence). Conditional recommendation, low-quality evidence).
In the plasma itself, 50% is ionised, 40% is plasma bound and 10% is chelated to various anions. There is a large gradient between the ionised calcium in the plasma and the tiny ionised fraction in the cells. So as an important starter, the serum level of calcium does not tell us much about overall levels in the body.
In broad terms we can compare dialysis (the movement of small molecules across a membrane along an osmotic gradient) with ultrafiltration (the squeezing of plasma through a big sieve that retains the big bits of the plasma and lets the other bits leak out). These rejoice in the acronyms CVVH, CVVHD and CVVHDF respectively.
Evaluate for retained products of conception as etiology Diagnosis Diagnosis of endometritis with at least two of the following: 8 Fever >100.4F Evaluate for retained products of conception as etiology Diagnosis Diagnosis of endometritis with at least two of the following: 8 Fever >100.4F
Up front there are some problems with the terminology * Plasmapheresis = process of removing plasma from the blood. Welcome back to the tasty morsels of critical care podcast. Plasmapheresis (or PLEX) is one of the machines we tend not to have responsibility for in the ICU. Unlike CRRT we tend to defer to another specialty to do this.
Through the years, we see a change to plasma, then crystalloid, and then 1:1:1 therapy. Once compared, while 1:1:1 therapy or giving PRBCs or plasma alone is better than crystalloid, whole blood is preferable and may have more of a survival benefit for patients. In the First World War, the preferred resuscitation fluid was whole blood.
Pro-inflammatory states may also play a role, as patients with CRPS have significantly higher levels of plasma cytokines and chemokines. What is Complex Regional Pain Syndrome? CRPS is distinguished from other chronic pain conditions by the presence of signs indicating prominent autonomic and inflammatory changes in the region of pain.
This is long episode, but there’s a TON of information…everything from tourniquets, pain management, blood vs. crystalloid, “scoop and run”, and much, much more. We also talk about education, and how The Church is looking to educate while still having a laugh or two. Dr. Fisher’s Twitter feed: [link] Kotwal, et al.
Results - A higher shock index score after arrival to the emergency department experienced longer hospital, intensive care unit, and mechanical ventilation days, injury severity scores, packed red blood cells, plasma, platelets, and total blood product usage. The shock index was calculated as heart rate/systolic blood pressure.
Plasmapheresis (which involves spinning the blood in a big machine until the plasma separates out, then removing all the plasma and replacing the volume with some 5% albumin and letting the body reproduce all the other plasma components itself) is another treatment supported by a 2012 Cochrane review of randomised trials.
Acute Aortic Dissection (AAD) A meta-analysis found that plasma D-dimer level <500 ng/mL is useful for identifying patients who are unlikely to have an AAD and do not require further aortic imaging. The chest pain started suddenly today while at rest, is located on the right side, and radiates to her back.
Have a look to see how their osmolarity and tonicity across the cell membrane compare to plasma. Renal (= urine output) : anti-diuretic hormone (ADH) release from the posterior pituitary is stimulated by microchanges in plasma osmolarity. This water is held in either the intracellular compartment (i.e. everywhere outside the cells).
Treatment consists of: * PLEX – actual proper PLEX with plasma replacement as opposed to just washing out all the good stuff and giving albumin as replacement. The plasma replacement replaces factors and reduces the bleeding risk (which is already high) but also acts as a source of ADAMSTS13.
Pregnancy itself with its bump in plasma volume, reduced Hb and increased cardiac output is like one long exercise stress test. Critical illness in pregnancy is remarkably rare given the somewhat bonkers system for reproduction that we seem to have evolved over the past million or years. Improved care of complex.
it is most commonly used for measuring heparin activity (which is a post in itself) but if the APTT is raised in in the absence of heparin then it might reflect factor deficiency (eg one of the thrombophilias) where it should correct to normal with a mixing study where normal plasma is added.
Internal potassium balance and the control of the plasma potassium concentration. Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. and/or in the presence of acute MI. Is 40 mEq too much? mEq/L to 3.0
In fact, there is laboratory evidence that CO toxicity increases Plateletneutrophil aggregates and plasma myeloperoxidase (MPO) concentration and thus may precipitate ACS (though this is by no means clinically proven). This was his ECG. Intravascular Neutrophil Activation Due to Carbon Monoxide Poisoning What do you think of this ECG?
Internal potassium balance and the control of the plasma potassium concentration. This is pathognomonic of hyperkalemia (I suppose it could be due to a massive overdose of a sodium channel blocking drug, maybe). Is it ventricular tachycardia (VT) due to hyperK or is it a supraventricular rhythm with hyperK? Is 40 mEq too much?
Peak plasma concentration of amphetamines is rapid ( within minutes ) following inhalation or injection. The estimated pulmonary artery systolic pressure is 29 mmHg + RA pressure. Conclusion: Type II MI probable due to hypoxia and tachycardia from resp arrest and amphetamine use.
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content