This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse McLaren illustrates the paradigm shift from STEMI to Occlusion MI (OMI) through 9 cases, and drives home the points that if there is STEMI criteria, consider false positives (eg. secondary and proportional to LVH or BER); if there is no STEMI criteria, consider false negatives and look for other signs of occlusion (eg.
Can you identify which were early repolarization and which were anterior STEMI? The post ECG Cases 2: Early Repolarization or Anterior STEMI? In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. appeared first on Emergency Medicine Cases.
The post ECG Cases 4: Lateral STEMI or Occlusion MI? In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Which had acute coronary occlusion? Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. We looked at 101 STEMI patients from two rural EDs. Date: November 22, 2023 Reference: Stopyra et al. AEM November 2023.
And for STEMI too. The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. Does heparin - LMWH or unfractionated heparin - benefit the patient with a pretty good story for angina with a bump in their troponin and some ST depression in the lateral leads? But should we? But should we?
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
We consider electrolyte disturbances and look for ECG signs of hyperkalemia or hypokalemia/hypomagnesemia, and we consider the differential of diffuse ST depression with reciprocal ST elevation in aVR, and false positive STEMI.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. This was sent to me by an undergraduate name Hans Helseth, who is an EKG tech, but who is an expert OMI ECG reader. He wrote most of it and I (Smith) edited.
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria.
Triage ECG: It was interpreted as lateral STEMI, and he was sent to the cath lab, where the angiogram showed unchanged CAD from known prior, with no acute culprit. Written by Pendell Meyers Two patients with acute chest pain. Do either, neither, or both have OMI and need reperfusion? Described as a dull ache, 6/10 in severity.
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
It does, in fact, the STE meets STEMI criteria since there is 1 mm of in V4 and V5. This ECG was texted to me with no other information. I assumed the presentation was consistent with acute MI. What did I say? Activate the cath lab." The T-waves in V2-V6 are diagnostic. There is also some non-diagnostic STE in inferior leads.
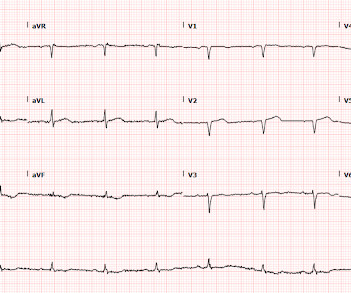
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
For instance, there was no protocol for stroke or STEMI. At some point along the way we had protocols for spinal motion restriction, alcohol withdrawal, stroke and STEMI, CPAP, and termination of cardiac arrest resuscitation on scene. There were fewer than 50 protocols in the book, along with pages for 24 medications and 8 procedures.
She knows the baseline is normal, and she knows the STEMI(-) OMI one is diagnostic of OMI, with the highest possible confidence. Here is the EM decision making: "The patient's EKG revealed some repolarization abnormalities but no clear signs of a STEMI. Back to the case: Unfortunately, the ECG was not understood by the provider.
Here they are: Patient 1, ECG1: Zoll computer algorithm stated: " STEMI , Anterior Infarct" Patient 2, ECG1: Zoll computer algorithm stated: "ST elevation, probably benign early repolarization." He diagnosed anterior "STEMI" and activated the cath lab. 25 minutes later, EMS called back with this new ECG: Super obvious STEMI(+) OMI.
link] == MY Comment, by K EN G RAUER, MD ( 8/6 /2023 ): == Brilliant talk by Dr. Smith on the state of the art addressing the “need for OMI — and the fallacy of STEMI”. The current STEMI paradigm that continues to be followed by all-too-many clinicians ( including all-too-many cardiologists ) is fallacious.
Subtle as a STEMI." (i.e., Here is the bottom line of the article: It is widely believed that hyperacute T-waves are a transitional state preceding ST Elevation 1–4 Thus, it is tempting to postulate that early cases of OMI will eventually evolve to STEMI; yet, our data contradicts that notion. This one is easy for the Queen.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
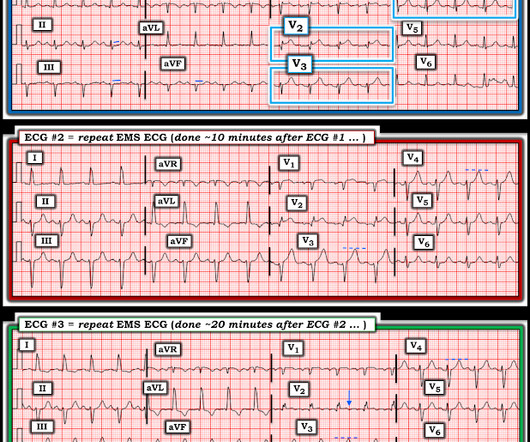
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. 2 Normal ECG #3. What was the outcome and final diagnosis?
If we took this as the gold standard, we would conclude that the computer interpretation was safe and accurate at least accurate enough to not miss STEMI, and that physicians should not be interrupted to interpret it, because there would be no change in patient management. What is the gold standard for ECG interpretation: patient outcome!!!
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He had a previous ECG on file: Proving the findings are new The cath lab was activated. He was given aspirin and sublingual nitro and the pain resolved.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
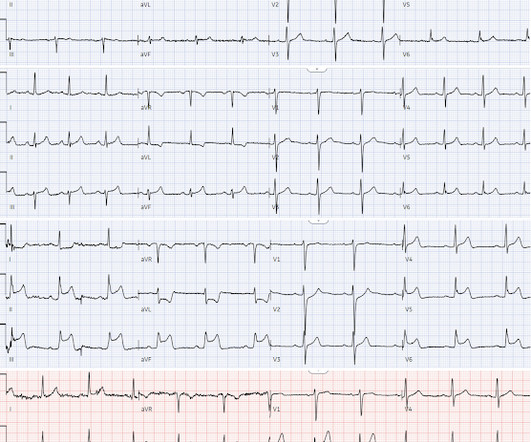
LVH produces secondary repolarization abnormalities that can mimic STEMI. Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves.
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen. As per My Comment in the above-cited Oct. 15, 2022 post — I like to focus on the ST-T wave appearance in leads V1 and V6 to facilitate recognition of Precordial Swirl.
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient. Could this false positive cath lab activation been prevented?
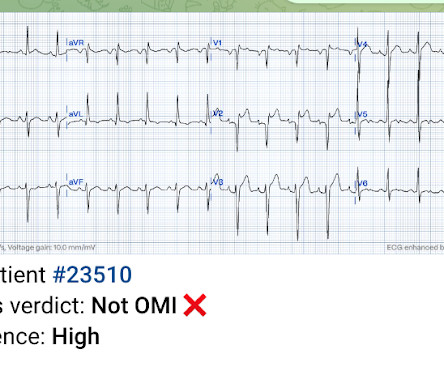
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. Do you need posterior leads? If so, how will they change management?
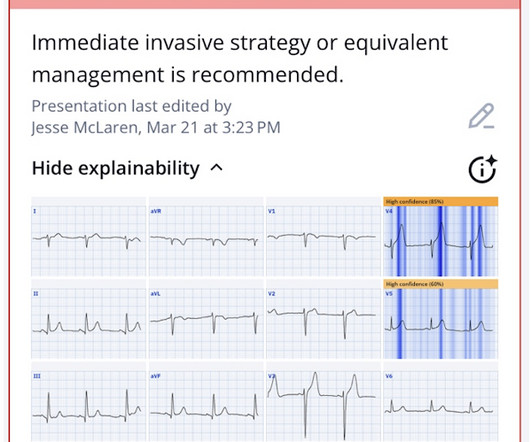
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Methods and Results Patients with confirmed ST elevation myocardial infarction (STEMI) treated by emergency medical services were included in this retrospective cohort analysis of the AVOID study. Greater severity of chest pain is presumed to be associated with a stronger likelihood of a true positive STEMI diagnosis.
So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. The patient was admitted as ‘NSTEMI’ which is supposed to represent a non-occlusive MI, but the underlying pathophysiology is analogous to a transient STEMI. See these posts: Chest Pain, ST Elevation, and an Elevated Troponin: Should we Activate the Cath Lab?
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
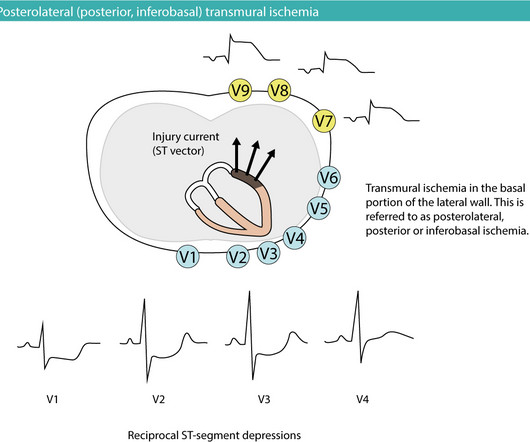
Posterior (posterolateral) acute myocardial infarction (STEMI) The heart is rotated 30° to the left in the thorax. The answer is rather simple: the probability that the patient has NSTE-ACS/NSTEMI is small and the vast majority has STE-ACS/STEMI. Leads V7–V9 must be placed to reveal the ST-segment elevations.
4,5] We have now formally studied this question: Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.[6] Written by Jesse McLaren Four patients presented with chest pain. have published a number of warnings about the previous reassuring studies.[4,5]
Unknown algorithm The Queen gets it right Case 4 How unreliable are computer algorithms in the Diagnosis of STEMI? The patient's prehospital ECG showed that there was massive STEMI and these are hyperacute T-waves "on the way down" as they normalize. It is not yet available, but this is your way to get on the list. 2 cases at once!
While STEMI negative, the ECG is diagnostic of proximal LAD occlusion. Transient STEMI” are often managed like non-STEMI with delayed angiography, which is very risky. This case is an example of the steps we can all take in daily practice as the paradigm shifts from STEMI to OMI.
We also studied 7 years of Code STEMI patients requiring emergent reperfusion, and found that 4% presented with an ECG labeled ‘normal’, often confirmed by the final blinded interpretation. Emergency department Code STEMI patients with initial electrocardiogram labeled ‘normal’ by computer interpretation: a 7-year retrospective review.
2: Human, Take this Patient to the Cath Lab – AI and STEMI Detection Spoon Feed These researchers developed and trained a deep ensemble artificial intelligence (AI) model to classify ECGs as STEMI versus non-STEMI. We always work hard, but we may not have time to read through a bunch of journals. It’s time to learn smarter.
In this ECG Cases blog, Jesse McLaren and Rajiv Thavanathan explore how ECG and POCUS complement each other for patients presenting to the emergency department with shortness of breath or chest pain. They explain complementary diagnostic insights into pericardial effusion and cardiac tamponade, occlusion MI and RV strain.
Discharge ECG showed antero-inferior reperfusion T wave inversion: Had the initial ECG been signed off as “STEMI negative” the patient could have arrested in the waiting room, with a poor cardiac and neurological outcome. A healthy 45-year-old female presented with chest pain, with normal vitals. What do you think? But which one is it?
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. The Case FIGURE 1: Initial EKG were notable for a leukocytosis of 23.19 Click to enlarge.)
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content