This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
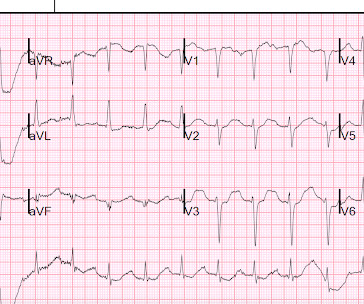
Here is his ED ECG: There is obvious infero-posterior STEMI. What are you worried about in addition to his STEMI? Comments: STEMI with hypokalemia, especially with a long QT, puts the patient at very high risk of Torsades or Ventricular fibrillation (see many references, with abstracts, below). There is atrial fibrillation.
Pregnancy itself with its bump in plasma volume, reduced Hb and increased cardiac output is like one long exercise stress test. While interesting and exam worthy you’re still going to see STEMI on the ECH and have to go to the cath lab so perhaps it doesn’t change much of what we do.
Discussion See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes I could find very little literature on the treatment of severe life-threatening hypokalemia. Internal potassium balance and the control of the plasma potassium concentration. and/or in the presence of acute MI. mEq/L to 3.0 mEq/L to 2.0
Internal potassium balance and the control of the plasma potassium concentration. to greatly decrease risk (although in STEMI, the optimal level is about 4.0-4.5 I could find very little literature on the treatment of severe life-threatening hypokalemia. The estimated deficit associated with a serum decrease from 4.0
In fact, there is laboratory evidence that CO toxicity increases Plateletneutrophil aggregates and plasma myeloperoxidase (MPO) concentration and thus may precipitate ACS (though this is by no means clinically proven). Intravascular Neutrophil Activation Due to Carbon Monoxide Poisoning What do you think of this ECG?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content