This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Jesse McLaren illustrates the paradigm shift from STEMI to Occlusion MI (OMI) through 9 cases, and drives home the points that if there is STEMI criteria, consider false positives (eg. secondary and proportional to LVH or BER); if there is no STEMI criteria, consider false negatives and look for other signs of occlusion (eg.
How can we use the awareness of complications to identify false positive STEMI and Occlusion MI that doesn’t meet classic STEMI criteria, and consider specific treatment? The post ECG Cases 41 – STEMI, Occlusion MI Complications appeared first on Emergency Medicine Cases.
To support EM Cases, please consider a donation here: [link] The post EM Quick Hits 57 – HIV Diagnosis, Failed Paradigm of STEMI Criteria, Poisoned Patient Airway Management, Spontaneous Bacterial Peritonitis, DIY Investments appeared first on Emergency Medicine Cases.
Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. Delayed First Medical Contact to Reperfusion Time Increases Mortality in Rural EMS Patients with STEMI. We looked at 101 STEMI patients from two rural EDs. Date: November 22, 2023 Reference: Stopyra et al. AEM November 2023.
And for STEMI too. The post JJ 16 Heparin for ACS and STEMI appeared first on Emergency Medicine Cases. We’re expected to routinely give heparin for all these NSTEMI and unstable angina patients with any ischemic changes seen on the ECG, right? But should we?
Can you identify which were early repolarization and which were anterior STEMI? The post ECG Cases 2: Early Repolarization or Anterior STEMI? In this ECG Cases blog we present ECGs from 7 patients who presented with chest pain and mild anterior ST elevation. appeared first on Emergency Medicine Cases.
In this ECG Cases blog we look at 9 patients with possible transient STEMI and discuss pitfalls and pearls in ECG interpretation and management. The post ECG Cases 39 – Transient STEMI Pitfalls and Pearls appeared first on Emergency Medicine Cases.
10 patients presented with the "STEMI-equivalent" ST elevation in aVR with diffuse ST depression. The post ECG cases 7: ST elevation in aVR, STEMI-equivalent? Which had acute coronary occlusion? Jesse McLaren guides us through the differential diagnosis of ST elevation in aVR with diffuse ST depression in this ECG Cases blog.
The post ECG Cases 4: Lateral STEMI or Occlusion MI? In this ECG Cases blog we look at seven patients with potentially ischemic symptoms and subtle ECG changes in the lateral leads. Which had acute coronary occlusion? Introducing the concept of Occlusion MI - a paradigm shift in ECG diagnosis of MI.
Jesse McLaren explains 'Late STEMI' and how reperfusion strategies should not be based on time of symptom onset. The post ECG Cases 25: ‘Late STEMI’ – How acute is the coronary occlusion? In this ECG Cases blog we look at 10 patients with potentially ischemic symptoms. appeared first on Emergency Medicine Cases.
A 60 yo with 2 previous inferior (RCA) STEMIs, stented, called 911 for one hour of chest pain. Here is his most recent previous ECG: This was recorded after intervention for inferior STEMI (with massive ST Elevation, see below), and shows inferior Q-waves with T-wave inversion typical of completed inferior OMI. ng/mL (quite large).
We discover that for STEMI/OMI vs subendocardial ischemia, we should look for STEMI(-)OMI, subacute OMI, and OMI in the presence of LBBB and RBBB, and consider the differential for diffuse ST depression with reciprocal ST elevation in aVR.
Traditionally, emergency providers looked for signs of ST-segment elevation myocardial infarction (STEMI) to indicate the need for intervention. Emergency physicians have recognized for some time that there are many occlusions of the coronary arteries that do not present with classic STEMI criteria on the ECG.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
The post EM Quick Hits 4 Acetaminophen Overdose & Warfarin Interaction, Dental Infections, MTP RABT Score, Statins for STEMI, Cricothyrotomy Tips appeared first on Emergency Medicine Cases.
We consider electrolyte disturbances and look for ECG signs of hyperkalemia or hypokalemia/hypomagnesemia, and we consider the differential of diffuse ST depression with reciprocal ST elevation in aVR, and false positive STEMI. The post ECG Cases 44 ECG Interpretation in Epigastric pain, Vomiting appeared first on Emergency Medicine Cases.
Doing so literally enables those of us who embrace the OMI Paradigm the ability to recognize within seconds that a patient with new CP ( C hest P ain ) — and — one or more hyperacute T waves — needs prompt cath regardless of potential absence of STEMI criteria.
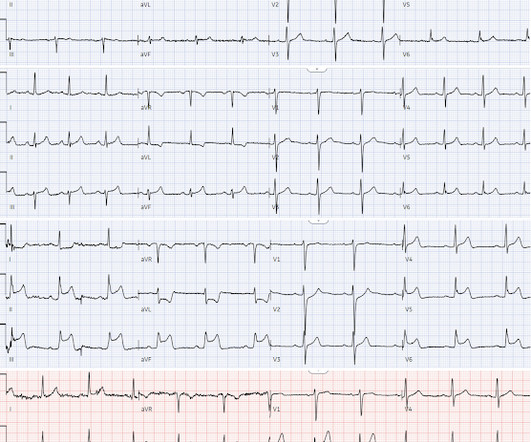
Theres ST elevation in V3-4 which meets STEMI criteria, which could be present in either early repolarization, pericarditis or injury. Lets see what happens in the current STEMI paradigm. Emergency physician: STEMI neg but with elevated troponin = Non-STEMI The first ECG was signed off. What do you think?
Interpretation : diagnostic of acute anterior OMI with STE less than STEMI criteria in V1-V4, hyperacute T waves in V2-V4, and suspiciously flat isoelectric ST segments in III and aVF suspicious for reciprocal findings. Now it even meets STEMI criteria, and HATWs continue to inflate. So the cath lab was not activated. Ongoing OMI.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
For instance, there was no protocol for stroke or STEMI. At some point along the way we had protocols for spinal motion restriction, alcohol withdrawal, stroke and STEMI, CPAP, and termination of cardiac arrest resuscitation on scene. The book was approved by the two largest hospitals in Hartford. Paramedics didnt do 12-lead ECGs then.
Cath lab declined as it is not a STEMI." And now this finding is even formally endorsed as a "STEMI equivalent" in the 2022 ACC guidelines!!! Another myocardial wall is sacrificed at the altar of the STEMI/NonSTEMI mindset. Do NOT give it unless you are committed to the cath lab!! Cath attending is aware. It is a mass delusion.
In this ECG Cases blog we review 8 cases of patients with prehospital ECGs and explore prehospital ECGs for diagnosing STEMI, Occlusion MI, false STEMI, code STEMI, dynamic ischemic changes, truncated voltages. Can you avoid the pitfalls and spot the pearls that help to make the diagnosis?
So while there’s no diagnostic STEMI criteria, there are multiple ischemic abnormalities in 11/12 leads involving QRS, ST and T waves, which are diagnostic of a proximal LAD occlusion. First trop was 7,000ng/L (normal 25% of ‘Non-STEMI’ patients with delayed angiography have the exact same pathology of acute coronary occlusion.
In patients with chest pain + ST elevation, consider false positive STEMI including early repolarization, LVH and Brugada-pattern. In patients with cocaine chest pain who are STEMI negative, beware STEMI(-)OMI including subtle ST elevation, hyperacute T waves, reciprocal change, and refractory ischemia.
Replace STEMI/NSTEMI with OMI/NOMI and AI in the ECG Diagnosis of OMI If you want to find it in the future, you can always find it at the banner above: I gave this Grand Rounds to UC Riverside a couple weeks ago. It is my most up to date lecture on OMI NOMI and Use of AI, especially the Queen of Hearts, in the Diagnosis of Occlusion MI.
The ECG did not meet STEMI criteria, and the final cardiology interpretation was “ST and T wave abnormality, consider anterior ischemia”. There’s only minimal ST elevation in III, which does not meet STEMI criteria of 1mm in two contiguous leads. But STEMI criteria is only 43% sensitive for OMI.[1]
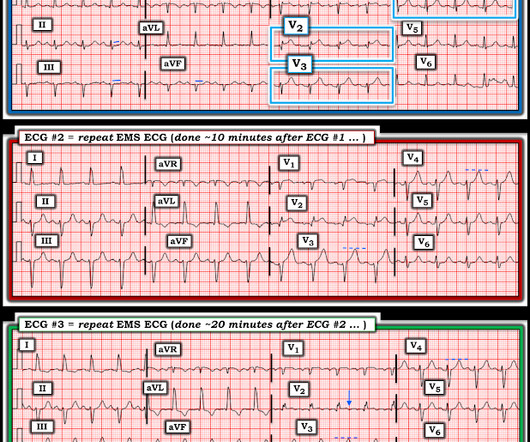
Obvious infero-postero-lateral STEMI(+)OMI, regardless of context Now let’s put them in order: what was the sequence? With serial ECGs that are ‘STEMI negative’ the physician could have waited for serial troponin levels or referred the patient as “non-STEMI”. What was the outcome and final diagnosis?
The biggest problem with STEMI criteria are false negatives – because this costs patient’s myocardium, with greater mortality and morbidity. For this reason, ECGs need first to be interpreted in isolation, and then applied to the patient. Could this false positive cath lab activation been prevented?
Despite anticipation by many that the initial post-resuscitation ECG will show an obvious acute infarction — this expected "STEMI picture" is often not seen.
This ECG was texted to me with the implied question "Is this a STEMI?": I responded that it is unlikely to be a STEMI. Septal STEMI often has ST depression in V5, V6, reciprocal to V1. Then combine with clinical presentation and low pretest probability 2 Saddleback STEMIs A Very Subtle LAD Occlusion.T-wave wave in V1??
In this ECG Cases blog we look at 8 patients with potentially ischemic symptoms, none of whom had STEMI on the 12 lead ECG. Which had occlusion MI? The post ECG cases 6: Posterior MI – Still Under-recognized appeared first on Emergency Medicine Cases.
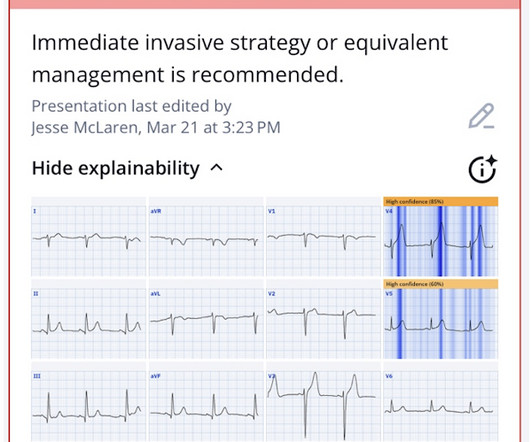
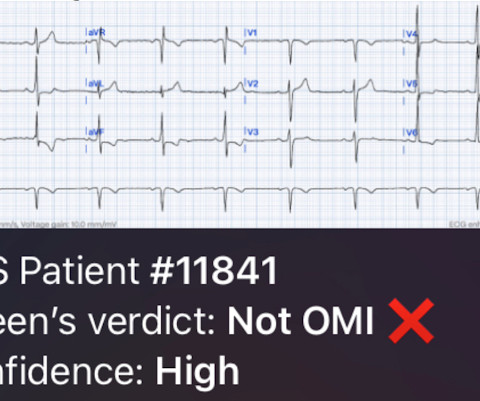
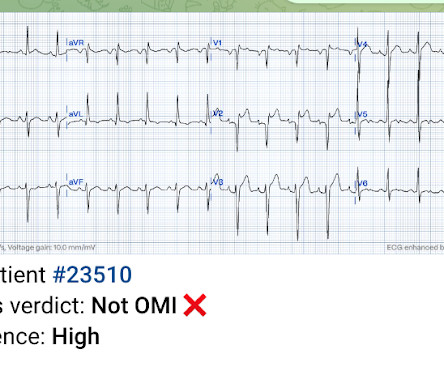
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
Seven patients with ischemic symptoms, none meeting STEMI criteria but all identified by a specific pattern of first diagonal branch occlusion are explored in this ECG Cases blog with Jesse MacLaren who also explains The South African Flag Sign.
If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. If it looks and feels like a STEMI clinically, get serial ECGs and consult Cardiology immediately. Take Home Points Provider assessment of how the patient looks is extremely important.
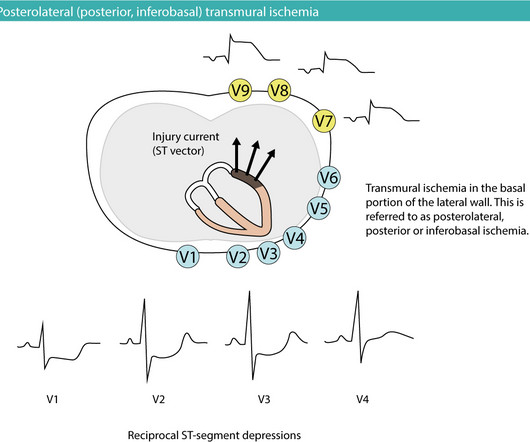
Posterior (posterolateral) acute myocardial infarction (STEMI) The heart is rotated 30° to the left in the thorax. The answer is rather simple: the probability that the patient has NSTE-ACS/NSTEMI is small and the vast majority has STE-ACS/STEMI. Leads V7–V9 must be placed to reveal the ST-segment elevations.
LVH produces secondary repolarization abnormalities that can mimic STEMI. Signs of occlusion MI in patients with LVH include: new Q waves/loss of R waves, disproportionate and dynamic ST elevation (or ST depression from posterior MI), and hyperacute T waves.
Many conditions outside of acute coronary syndrome (ACS) mimic ST-elevation myocardial infarction (STEMI), but only a handful of cases have reported ST-elevations (STE) in the setting of pancreatic inflammation where underlying ACS was excluded. Mimics of ST elevation myocardial infarction (STEMI). Accessed November 29, 2023.
Posterior leads are unnecessary if anterior leads are diagnostic According to the STEMI paradigm an ECG has to have ST elevation to diagnose acute coronary occlusion, and if there’s no ST elevation on anterior leads you can look for it on posterior leads. Do you need posterior leads? If so, how will they change management?
We organize all of the trending information in your field so you don't have to. Join 5,000+ users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.































Let's personalize your content